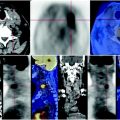
Fig. 23.1
Presence of some lymph nodes in the left para-aortic region that compress the pyeloureteral junction without causing obstruction (MIP image)
23.4 Conclusions
The PET scan shows extended locoregional recurrence associated with nodal satellite involvement that is responsible for right lower limb plexopathy and ipsilateral obstructive uropathy.
The sequence of images (Figs. 23.2, 23.3, 23.4, 23.5, 23.6) shows the morpho-functional dissociation: at the CT, the right kidney is increased in size but has slight parenchymal function. Cortical thickness is slightly thinned (Fig. 23.2, red arrows), the pelvis is severely dilated and has a predominantly exophytic development. We observe the presence of contrast administered during a CT scan performed a few days before (Fig. 23.2, yellow arrows), for the same reason contrast can be seen in the bowel (Fig. 23.2, blue arrows). The PET shows weak deposition of glucose in the right renal cortex (Fig. 23.2, red arrows), while there is absent activity in the excretory cavity (Fig. 23.2, yellow arrows). This item indicates the limited function of the parenchyma and poor filtration caused by the tumoral obstructive ureteral infiltration. The parenchymal concentration of glucose is not predictive of recovery of renal function, after the obstruction was removed with a stent implantation.

 Laryngeal Squamous Carcinoma: Staging
Laryngeal Squamous Carcinoma: Staging
 Radio-Treated Cancer of the Posterior Hemi-Circumference of the Anal Canal: Post-Actinic Fibrosis
Radio-Treated Cancer of the Posterior Hemi-Circumference of the Anal Canal: Post-Actinic Fibrosis
 Bone-Destroying Metastases in Thyroid Undifferentiated Carcinoma
Bone-Destroying Metastases in Thyroid Undifferentiated Carcinoma
 Surgically Treated Endometrial Cancer: Bilateral Nodal Recurrence
Surgically Treated Endometrial Cancer: Bilateral Nodal Recurrence
 Undifferentiated Gastric Adenocarcinoma with Peritoneal Carcinosis
Undifferentiated Gastric Adenocarcinoma with Peritoneal Carcinosis
 Follow-Up of Papillary Breast Cancer: Solitary Sacroiliac Benign Lesion
Follow-Up of Papillary Breast Cancer: Solitary Sacroiliac Benign Lesion




Related posts:
Laryngeal Squamous Carcinoma: Staging
Radio-Treated Cancer of the Posterior Hemi-Circumference of the Anal Canal: Post-Actinic Fibrosis
Bone-Destroying Metastases in Thyroid Undifferentiated Carcinoma
Surgically Treated Endometrial Cancer: Bilateral Nodal Recurrence
Undifferentiated Gastric Adenocarcinoma with Peritoneal Carcinosis
Follow-Up of Papillary Breast Cancer: Solitary Sacroiliac Benign Lesion
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
