
Case 8-01. Tibial shaft fracture. AP radiograph of the leg. There is a transverse fracture of the tibial shaft with a butterfly fragment on the lateral side, indicative of a fracture caused by bending. The convex side of the bend corresponds to the site of the transverse portion of the fracture, and is indicative of loading under tension. The concave side of the bend corresponds to the butterfly fragment, and is indicative of loading under compression. There is a transverse fracture of the fibular shaft at the same level.


Case 8-02. Tibial shaft fracture. AP and Lateral radiographs of the lower leg. There is a spiral fracture of the distal tibial shaft. The fracture line spirals around the full circumference of the tibial shaft, with the two ends joined by a vertical component. This fracture is the result of loading under torsion (twisting force). A closed tibial shaft fracture such as this may be treated with a locked intramedullary rod [1].


Case 8-03. Gunshot wound. AP and Lateral radiographs of the lower leg. There is a gunshot wound involving the tibia and fibula. The pattern of fractures is indicative of a low velocity projectile, such as from a hand gun, with an entry wound from the posterior aspect. (The victim was shot in the back of the leg by a handgun.) Gunshot wounds are open fractures and carry a significant risk of infection. Treatment often includes debridement, external fixation, and antibiotic beads [2].

Case 8-04. Gunshot wound. AP and Lateral radiographs of the lower leg. There is a gunshot wound involving the shaft of the fibula. The pattern of fractures is indicative of a low velocity projectile, such as from a hand gun, with tissue damage confined to the path of the bullet and the fragments of bone that acted as secondary projectiles.


Case 8-05. Segmental tibial and fibular shaft fractures. AP and Lateral radiographs of the leg. There are segmental fractures of the tibial and fibular shafts. Note that the knee and ankle are pointing in different directions. There is an old, healed ankle fracture with internal fixation. Segmental fractures are the result of high-energy trauma and may be treated by a variety of means, including intramedullary rods, internal fixation, and external fixation [3].


Case 8-06. Open fractures of the tibia. Lateral and AP radiographs of the lower leg. There are comminuted open fractures of the tibial shaft, with gas in the soft tissues. Open fractures carry a significant risk of infection [2].


Case 8-07. Tibial and fibular shaft fractures. Lateral and AP radiographs of the lower leg. There are comminuted transverse fractures of the distal tibial and fibular shafts with lateral angulation of the distal fragments.


Case 8-08. Stress fracture. Lateral and AP radiographs of the lower leg. There is a partially healed stress fracture of the tibia, best seen on the lateral view as a transverse line that extend partway across the anterior cortex. Heaped periosteal bone formation adjacent to the fracture line is the result of the healing process.
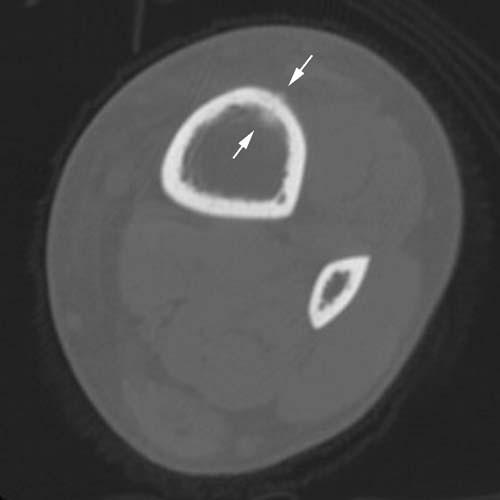
Case 8-09. Longitudinal stress fracture. Runner with leg pain. Axial CT slice of the proximal third of the tibial shaft. There is a longitudinal fracture of the anterior tibial cortex with evidence of periosteal and endosteal healing (arrows). Longitudinal stress fractures are relatively uncommon [4-6].
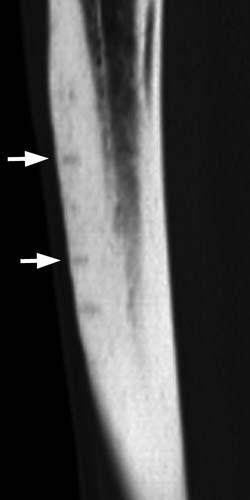
Case 8-10. Multiple stress fractures. Runner with recurrent leg pain. Sagittal CT reformatted image. There are multiple stress fractures in the anterior tibial cortex seen as short horizontal lines extending partway across the cortex. Two of them are indicated by arrows, but more are present. Most stress fractures may be managed by rest and activity modification; in some circumstances, intramedullary rod placement may be appropriate for a more rapid return to activity [7].


Case 8-11. Toddler’s fracture. AP and lateral radiographs of the lower leg in a 3-year-old child. There is a minimally displaced spiral fracture of the distal tibial shaft, a so-called toddlers fracture from falling while learning to walk [8]. Toddlers fractures are often difficult to demonstrate by radiographs. It is important to distinguish toddlers fractures from fractures caused by non-accidental trauma [9].

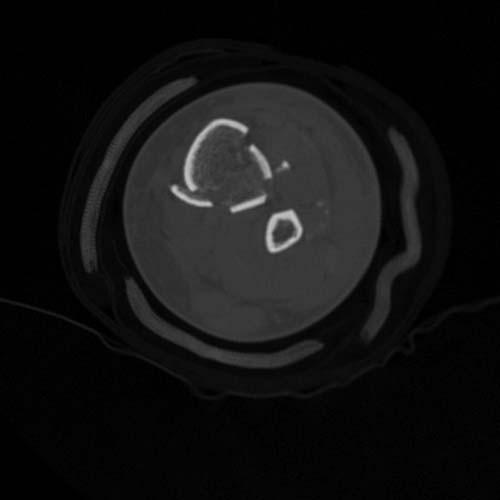
Case 8-12.
Pilon fracture. Motor vehicle crash. AP radiograph of the lower leg shows a comminuted fracture of the tibia that extends from the joint line of the ankle proximally into the shaft. There is an accompanying distal fibular shaft fracture.


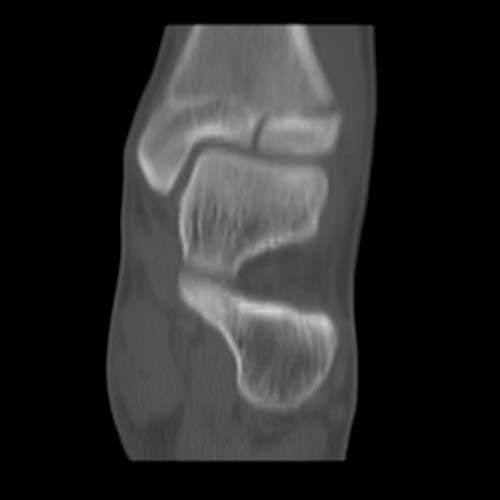
Coronal and Sagittal CT reformatted images, after an external fixator has been applied, show the severe comminution and the involvement of the articular surface and distal metaphysis of the tibia.
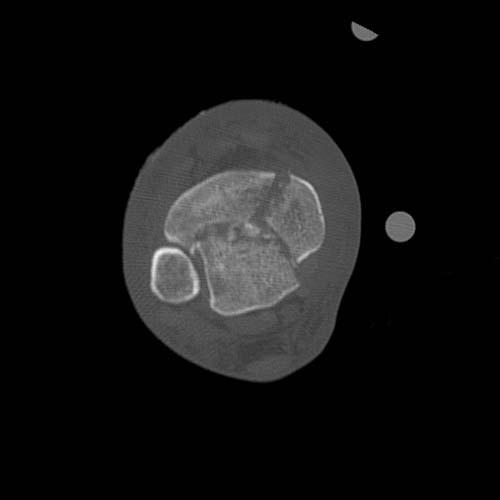
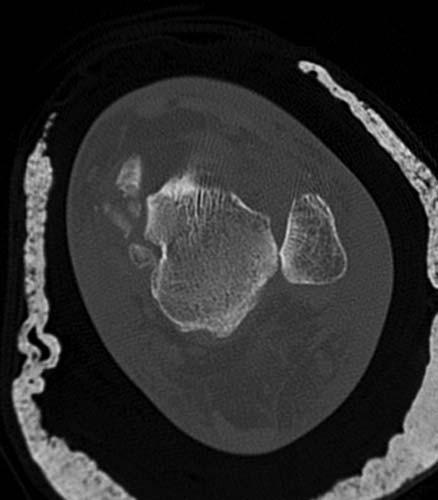
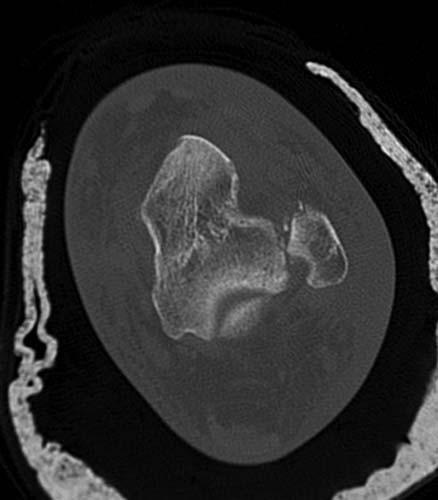
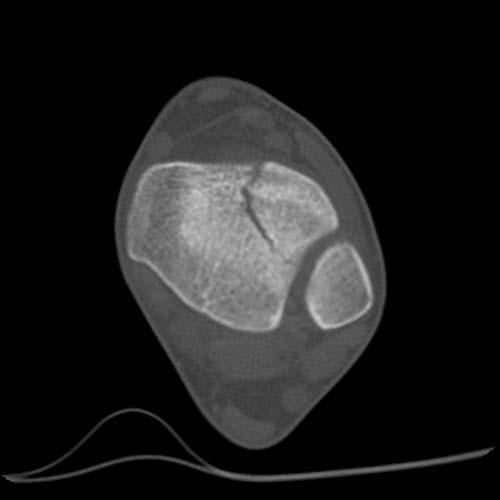
Axial CT slice through the distal tibia shows a characteristic fracture pattern, with anterior, posterior, and medial major fragments, and central comminution. This injury is called a pilon fracture, and is the result of severe axial compression that is transmitted through the foot and ankle joint to the distal tibia [10-11]. A common circumstance for this fracture is an automobile crash where the feet are braced against the floorboard at the moment of impact.


Case 8-13. Pilon fracture. AP and Lateral radiographs show a severely angulated comminuted fracture of the distal tibial and fibular shafts with extension to the tibial articular surface.



Coronal CT reformatted images, following initial closed reduction show the comminution and involvement of the articular surface.




Sagittal CT reformatted images, following initial closed reduction show the comminution and involvement of the articular surface.
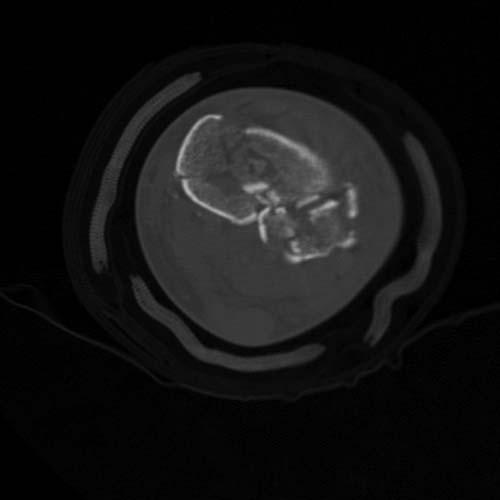
Axial CT images show severe comminution of the tibia.



Case 8-14. Pilon fracture. 85-year-old woman injured in a high speed motor vehicle crash. AP, Mortise, and Lateral radiographs of the ankle show an intra-articular fracture of the distal tibia in the coronal plane. There is an avulsion fracture of the tip of the medial malleolus, and the medial ankle mortise is widened. There is extensive soft tissue swelling.
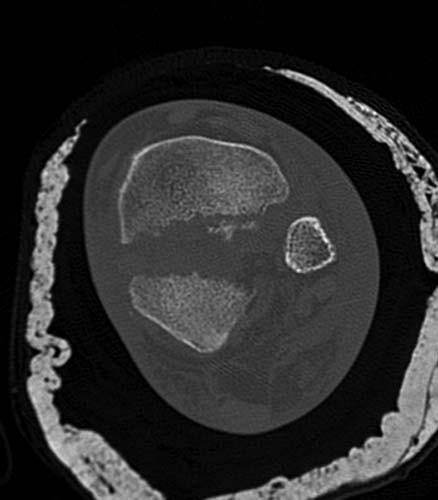
Axial CT slice at the distal tibia shows the displaced intra-articular fracture of the tibia in the coronal plane and dislocation of the distal tibio-fibular joint.
Axial CT slice through the malleoli shows fractures of the medial malleoli and subluxation of the talus relative to the lateral malleolus.
Axial CT through the tip of the lateral malleolus shows small avulsion fragments from the anterior aspect of the fibula and possibility from the talus.

Axial CT through the calcaneal cuboid joint shows medial subluxation of the cuboid relative to the calcaneus, and a small avulsion fracture of the distal lateral margin of the calcaneus; both findings suggest capsular disruption of the calcaneal cuboid joint.
Axial CT through the os peroneum shows fragmentation, consistent with peroneal tendon injury.

Sagittal CT reformation shows the distal tibial fracture in the coronal plane with displacement of the dome of the talus between the fragments.


Sagittal and Coronal CT reformations show minimally displaced fracture of the lateral process of the talus.


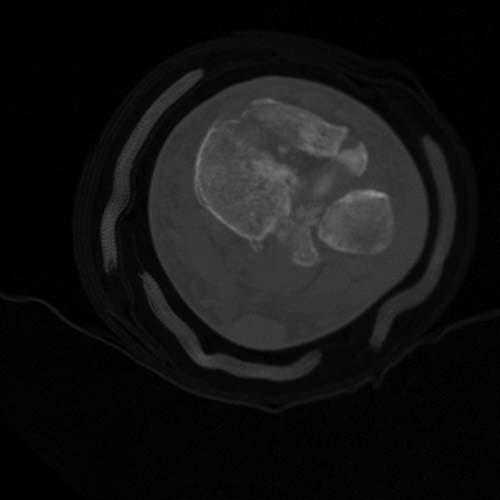
Case 8-15. Pilon fracture. 35-year-old man injured as a pedestrian struck by a car. AP and Lateral radiographs of the lower leg show a comminuted fracture of the distal tibial shaft with an intra-articular component extending to the ankle joint.

Axial CT slice at the distal tibia shows a mildly displaced intra-articular fracture of the tibial plafond dividing it into anterolateral and posteromedial fragments.


Coronal and Sagittal CT images show the distal intra-articular fracture line without step-off at the articular surface.



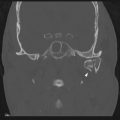
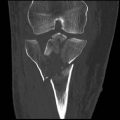
Case 8-16. Triplane fracture. 15-year-old adolescent male. AP and Mortise radiographs of the ankle show a fracture in the sagittal plane through the distal tibial epiphysis and widening of the lateral portion of the physis (growth plate). Lateral radiograph shows a fracture in the coronal plane extending from the partially closed physis through the posterior aspect of the distal tibial metaphysis. Because the fracture is oriented in the sagittal, axial, and coronal planes, it is called a triplane fracture. This fracture can only occur when the physis is partially closed, so the age of vulnerability is narrow [12]. This fracture is classified as a Salter type IV.


Sagittal and Coronal CT reformations show the fracture planes.



Three different perspectives of the surface rendered 3-D CT reconstruction show the triplane fracture.

Case 8-17. Lateral ankle sprain. AP radiograph of the left ankle shows soft tissue swelling over the lateral malleolus, more evident when the medial and lateral sides are compared. No fracture is present. This appearance indicates a lateral ankle sprain, and usually corresponds to a tear of the anterior talofibular ligament. This young man injured his ankle playing football, and heard a popping sound at the moment of injury.



Case 8-18. Oblique lateral malleolar fracture. AP, Mortise, and Lateral radiographs of the right ankle. There is an oblique fracture of the distal fibula, extending from the posterior cortex inferiorly to the anterior cortex. The fracture extends to the level of the tibial plafond. There is overlying soft tissue swelling. The distal fragment is only mildly displaced. This is the most common type of ankle fracture. The Danis-Weber system focuses exclusively on the level of the fibular fracture [13-15]. An ankle fracture in which the fibular fracture extends below the ankle joint (tibio-talar joint) is classified as a Weber A. If the fibular fracture is at the level of the joint but not below, it is a Weber B. If the fibular fracture is entirely above the joint, it is a Weber C. If there is no fibular fracture, the classification system does not apply. This case would be classified as a Weber B.


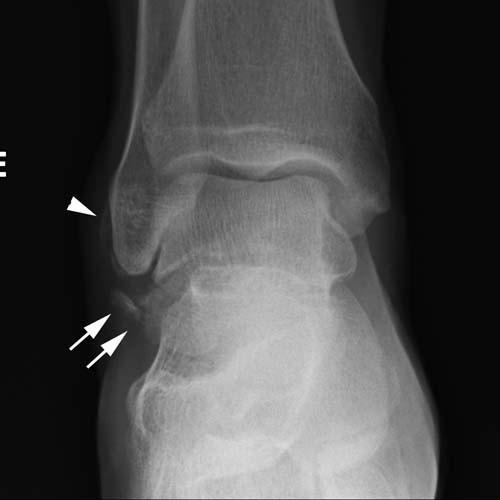
Case 8-19. Transverse lateral malleolar avulsion fracture. Mortise and lateral radiographs of the left ankle. There is a transverse fracture at the tip of the lateral malleolus, indicative of an avulsion by the lateral collateral ligament. The fragment is only mildly displaced. The overlying soft tissues are swollen. This fracture could be classified as a Weber A. An alternative system for classification is the Lauge-Hansen classification, which relates the position of the foot and the loading of the talus to the fractures. This system was derived from work that reproduced various ankle fractures in cadaver limbs [16-20]. Unlike the Weber classification, the Lauge-Hansen system incorporates the severity of the injury and the presence of injury without fracture. This fracture would be classified as a supination-adduction injury, stage 1. Supination of the foot and adduction of the talus as the mode of loading may also be called inversion. In a stage 2 supination-adduction injury, the medial malleolus is also fractured.



Case 8-20. Lateral malleolar fracture with medial ligamentous injury. AP, Mortise, and Lateral radiographs of the ankle. There is an oblique fracture of the distal fibula with minimal displacement. The fracture extends from the posterior cortex inferiorly to the level of the tibial plafond. The overlying soft tissues are swollen, but the ankle mortise appears intact. This injury could be classified as a Weber B.

AP passive stress radiograph shows lateral displacement of the distal fragment, lateral shift of the talus within the ankle mortise, and widening of the space (arrow) between the talus and the medial malleolus. This widening indicates that the deltoid ligament is torn, and that the ankle is unstable. The deltoid ligament attaches the medial malleolus to the talus and calcaneus. The passive radiograph is obtained by laying the patient on the injured side and placing a cushion underneath the leg. The foot and ankle dangle over the end of the cushion, and the weight of the foot provides the stress. The arrowheads indicated the direction of the stress. A horizontal x-ray beam is used to expose the radiograph. According to the Lauge-Hansen system, this injury would be classified as pronation-abduction, stage 3.



Case 8-21. Distal fibular shaft fracture. AP, Mortise, and Lateral radiographs of the left ankle. There is a laterally displaced oblique fracture of the distal fibular shaft that ends above the level of the distal tibio-fibular syndesmosis. The syndesmosis itself is widened, consistent with ligamentous disruption, and the talus is shifted laterally with respect to the tibia, consistent with rupture of the deltoid ligament. This fracture could be classified as a Weber C. Using the Lauge-Hansen system, this injury would be classified as pronation-eversion, stage 3 or 4.




Case 8-22. Maisonneuve fracture. AP, Mortise, and Lateral radiographs of the right ankle. There is a high fibular shaft fracture. There is lateral displacement and dislocation of the distal tibio-fibular syndesmosis, consistent with ligamentous rupture of the anterior and posterior tibiofibular ligaments and tear of the interosseous membrane distally from the level of the fibular fracture. The talus has shifted laterally within the ankle mortise, indicative of rupture of the deltoid ligament. This injury complex is called a Maisonneuve fracture. This could have the Lauge-Hansen classification of pronation-eversion, stage 4, or Weber C.



Case 8-23. Medial malleolar fracture. AP, Mortise, and Lateral radiographs. There is a transverse fracture through the medial malleolus at the level of the tibial plafond. The fracture is mildly displaced. Without a fibular fracture, the Danis-Weber classification cannot be used. In the Lauge-Hansen system, this could be classified as a pronation-abduction, stage 1 or 2.



Case 8-24. Medial malleolar fracture. AP, Mortise, and Lateral radiographs. There is an oblique fracture of the medial malleolus extending proximally and laterally from the tibial plafond. Without a fibular fracture, the Danis-Weber classification cannot be used. In the Lauge-Hansen system, this could be classified as a supination-adduction, stage 2.



Case 8-25. Medial malleolar fracture. AP, Mortise, and Lateral radiographs. There is a fracture of the medial malleolus extending through the partially closed medial physis distally through the epiphysis. This is a Salter type III fracture.



Case 8-26. Trimalleolar ankle fracture. AP, Mortise, and Lateral radiographs. There is a transverse fracture of the medial malleolus at the level of the tibial plafond with lateral displacement; the malleolar fragment is apposed to the talus, which is shifted laterally, indicating that the deltoid ligament is intact. There is a lateral displaced and angulated fracture of the distal fibula extending from the posterior aspect of the shaft distally and anteriorly to the level of the tibial plafond. The lateral malleolar fragment is apposed to the talus, indicating that the lateral collateral ligaments are intact. The lateral radiograph shows a small posterior malleolar fragment that has displaced with the lateral malleolar fragment. The syndesmosis is widened. This injury could be classified as a pronation-abduction ankle fracture, stage 3.
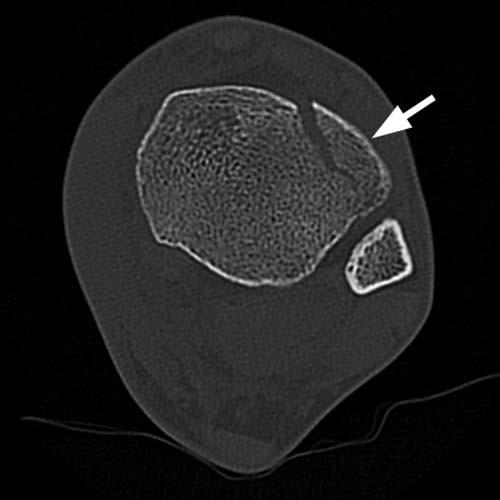
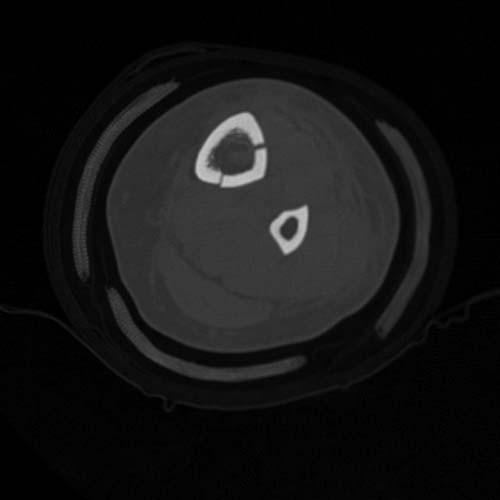
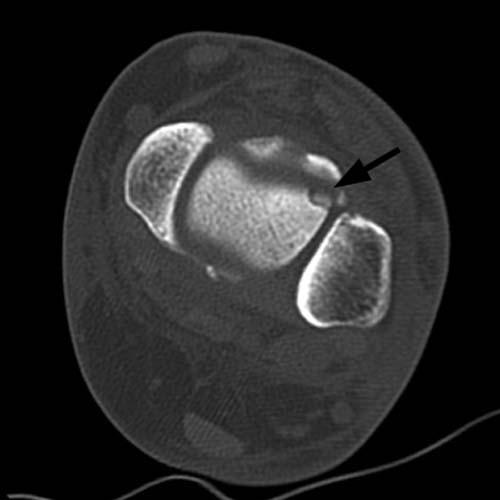
Case 8-27. Adult Tillaux fracture. Axial CT slice of the left ankle at the level of the syndesmosis. There is an avulsion fracture of the anterolateral margin of the distal tibia (arrow). The Tillaux fracture is an avulsion fracture of the anterolateral tibia at the attachment of the anterior tibiofibular ligament [21].
Case 8-28. Juvenile Tillaux fracture. Axial CT slice at the level of the syndesmosis. There is a mildly displaced fracture of the anterior lateral corner of the distal tibia. Coronal CT reformation shows the fracture planes extending in the axial plane through the lateral portion of the physis and in the sagittal plane through the epiphysis. The physis is partially closed. This is a Salter type III fracture that only occurs when the physis is partially closed [21].

Case 8-29. Open ankle fracture. Lateral ankle radiograph. Fractures of the medial malleolus and distal fibular shaft are evident. Gas is present within the ankle joint (arrow), indicative of an open fracture.


Case 8-30. Ankle fracture-dislocation. AP and Lateral radiographs. There is a grossly displaced fracture of the distal fibula with posterolateral dislocation of the foot from the ankle mortise.
Chapter 9. Foot
by Hyojeong Mulcahy, M.D., and Felix S. Chew, M.D.


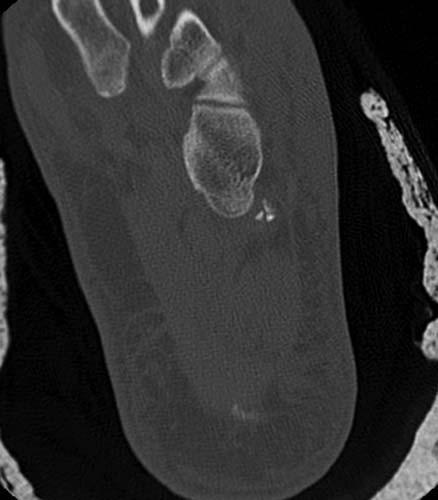
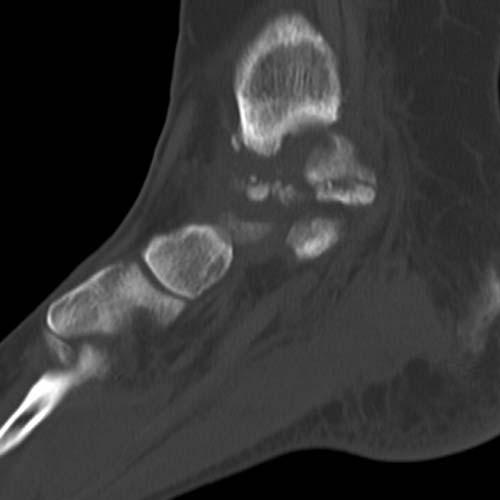
Case 9-01. Talar body fracture-dislocation. Lateral radiograph and corresponding 2D sagittal CT image of the talus demonstrate a fracture through the body of talus with subtalar dislocation. The posterior facet of calcaneus is dislocated anteriorly (arrow in A and B). The alignment of tibiotalar and the talonavicular joints is preserved. The blood supply of the talar dome typically enters distally and courses proximally. Therefore, fractures across the waist of the talus carry a risk for posttraumatic osteonecrosis of the talar dome, similar to the situation with the scaphoid and the femoral neck [1].

Case 9-02. Talar extrusion from 30-foot fall. 2D coronal CT image of the ankle demonstrates partial talar extrusion. The talus is dislocated medially from the ankle mortise and also from the subtalar joint. There is moderate internal rotation and medial displacement of talus. The anterior medial aspect of the talus extrudes through the soft tissues of the medial ankle and through an open defect in the skin (arrow). Accordingly, there is large amount of air within the ankle joint. Open talar fractures with extrusion of the talar body or the entire talus are typically the result of high-energy trauma and are frequently associated with markedly displaced fractures, severe soft-tissue injury, contamination, and disruption of the talar blood supply [1-2].


Case 9-03. Osteochondral defect of talus. Axial, 2D sagittal, and 2D coronal CT images of the ankle demonstrate a small osteochondral defect at the anterolateral aspect of the talar dome (arrow in A, B, and C). The fragment is completely detached from the talar dome, however, it is in situ (stage III). The classification of osteochondral defect was devised by Berndt and Harty. Stage I lesions are compression of the talar dome with no associated ligament ruptures and intact cartilage. Stage II lesions are incomplete fractures with the fragment remaining partially detached. Stage III lesions are complete fractures but not displaced. Stage IV lesions are detached [3-4].


Case 9-04. Lateral process of talus fracture after 20-foot fall. Lateral, mortise, and AP radiographs of the ankle demonstrates a comminuted lateral process of talus fracture type III (arrows). There is diffuse soft tissue swelling. There is peroneal sleeve avulsion fracture at the lateral malleolus (arrowheads).

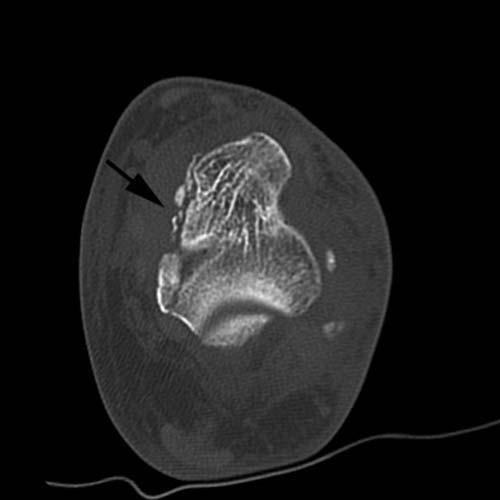
Axial and 2D sagittal, CT images of the ankle demonstrate a large comminuted fracture of the lateral process of the talus, which extends into the anterior medial aspect of the posterior facet. Minimal fracture extension into the posterior lateral aspect of the posterior facet is also noted (arrow in E). The lateral process of the body of the talus is a broad-based wedge-shaped prominence that articulates dorsolaterally with the fibula and inferomedially with the os calcis, thereby forming the lateral part of the subtalar joint. Fracture of the lateral process is seen typically in snowboarders. Before the development of this sport, these fractures were rare and generally associated with motor vehicle accidents, falls from a height, or simple inversion injuries. With the increasing popularity of snowboarding, fractures of the lateral process of the talus occur more frequently and account for 2.3% of snowboarding injuries. According to Hawkins, these fractures may be classified as non-articular (type I), a single fragment involving the talofibular articulation and subtalar joint (type II), and comminuted fractures, also involving both articulations (type III). Fracture of the lateral process of the talus has often been misdiagnosed as a lateral ankle sprain. The sequelae of missed fractures, particularly types II and III, include malunion, nonunion, long-term disability and degenerative arthritis of the subtalar joint [5-7].

Case 9-05. Talus avulsion fractures from motor vehicle accident. Lateral ankle radiograph demonstrates scale-like dorsal avulsion fracture of talar neck (arrow). This is the most common site of talar avulsion injury at the point of attachment of the ankle joint capsule [7].

Axial CT images demonstrate a mildly comminuted fracture involving the medial margin of the talus with minimal displacement (arrow in B) and a minimally displaced fracture of the medial aspect of the navicular and a small avulsion fragment.


Coronal CT images show talar medial process avulsion fractures (arrow).

Sagittal CT images show lateral malleolar avulsion fracture (arrow in F) and medial talar fractures (G).

Sagittal CT images show a minimally displaced fracture of the medial aspect of the navicular (arrow).



Case 9-06. Talus fracture-dislocation. AP, oblique, and lateral radiograph of the ankle shows laterally dislocated talus at the tibiotalar and subtalar joints. There is a fracture through the talar neck (arrow in C). This is a Hawkins type III talar neck fracture-dislocation. Avascular necrosis and/or degenerative arthritis can be expected in over 50% of cases. Avascular necrosis usually becomes evident on routine radiographs in 6 to 8 weeks. During this non-weight bearing period, disuse osteoporosis develops that leads to subchondral lucency in the talar dome. This finding( Hawkins sign) indicates intact vascular supply [8].


Case 9-07. Medial subtalar dislocation. Lateral radiograph of the ankle shows posterior displacement of the calcaneus with respect to the talus at the subtalar joint (long arrow in A). The talonavicular joint is not seen well on the lateral view (short arrow in A). AP radiograph of the ankle demonstrates unopposed head of the talus (arrow in B), and medially dislocated navicular and the remainder of the foot. The tibiotalar alignment is preserved.

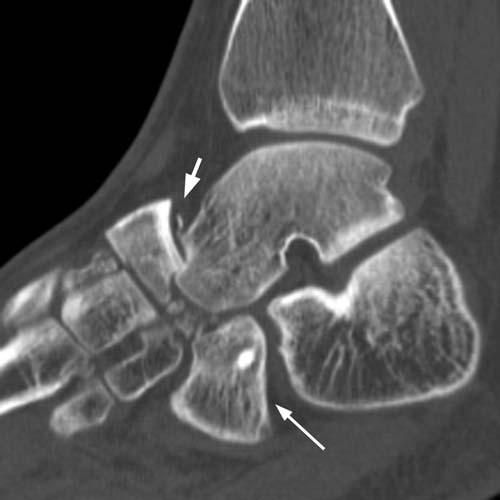
Case 9-08. Calcaneal compression fracture-centrolateral compression type after stepped down a curb. Lateral ankle radiograph demonstrates the fracture line exiting vertically just posterior to the posterior subtalar facet (arrow). The principal fragment containing the posterior facet is separated from the tuberosity by a vertical fracture line just posterior to the posterior facet. This is a centrolateral compression type.


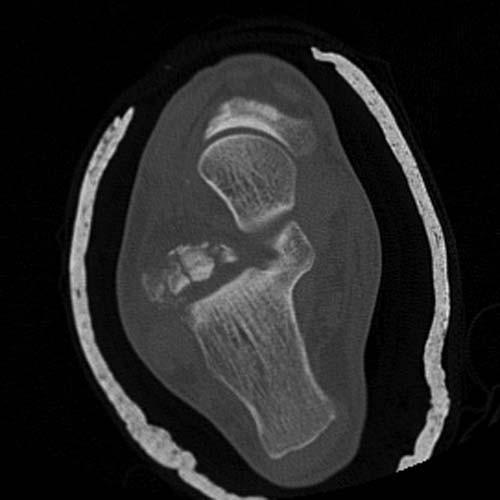
2D sagittal and axial CT images show an axial load comminuted compression fracture with impaction of the posterior calcaneus into the body of the calcaneus(arrow in B), extension of fracture lines into the calcaneocuboid articulation, into the sustentaculum tali and into the posterior subtalar articulation. There is rotation of the posterior lateral calcaneal fragment resulting in widening of the lateral aspect of the posterior subtalar joint (arrow in C).

Case 9-09. Calcaneal compression fracture-tongue type. Lateral radiograph of ankle demonstrates an impacted calcaneal fracture with the fracture line vertically extending to the posterior facet, and horizontally extending to the tuberosity (arrow). The principal fragment of the posterior facet contains the upper portion of the tuberosity, and this fragment has a tongue-like appearance and thus designated as tongue type.


Case 9-10. Calcaneus anterior process fracture. Lateral radiograph and oblique of the foot. There is a minimally displaced fracture at the anterior process of calcaneus (arrows). Fractures of the anterior process are the most common form of avulsion fracture of the calcaneus. The anterior process serves as the attachment of the bifurcate ligament. This ligament extends from the anterior process in two limbs, one attaching to the lateral portion of the navicular bone and the other to the adjoining surface of the cuboid bone. The fracture is best seen on oblique views and may not be seen on anteroposterior and lateral views.


Case 9-11. Calcaneus anterior process fracture non-union with a remote history of trauma. Lateral radiograph and 2D sagittal CT image ( B) of the ankle. There is a minimally displaced fracture at the anterior process of calcaneus with cortication of fracture margin indicating non-union (arrow in A and B). CT is particularly helpful for evaluation of anterior process fractures. Nonunion is the most common complication [9].

Case 9-12. Chopart fracture dislocation from bike accident. AP radiograph and 2D sagittal CT image of the foot demonstrate a fracture of the lateral navicular bone, with medial dislocation of the navicular bone with respect to the talar head (arrow head in A), and medial dislocation of the cuboid with respect to the calcaneus (arrow in A). There is impaction of the superomedial aspect of the talar head by fragments of the navicular, with a small cortical fragment avulsed and superiorly displaced (short arrow in B). In addition there is a minimally comminuted longitudinal fracture of the proximal middle cuneiform, and a small fracture on the dorsal aspect of the proximal cuboid. There is medial and inferior dislocation of the talus at talonavicular joint and the calcaneus at the calcaneocuboid joint with widening of the calcaneocuboidal joint (long arrow in B). The subtalar joint alignment is preserved. Findings are consistent with Chopart fracture dislocation. The joint between the hindfoot, and the midfoot, composed of the talonavicular and calcaneocuboid joints, is referred to as the Chopart joint.

Case 9-13. Navicular horizontal fracture. An oblique radiograph of the foot. There is a horizontal fracture of the navicular (arrow) with mild dorsal dislocation of the anterior fragment at the naviculocuneiform joint (arrow head). The fracture extends to the talonavicular and naviculocuneiform joint space.



Case 9-14. Navicular fracture-dislocation from 40-foot fall. AP, oblique, and lateral radiographs of the foot. There is a minimally displaced fracture involving the tuberosity and the body of the navicular bone with comminution at the lateral aspect. There is medial and dorsal dislocation of the navicular with respect to the talus at the talonavicular joint (long and medium arrows). This has been termed a swivel dislocation. There is medial or, less commonly, lateral dislocation of the talonavicular joint. There is only minimal subluxation of the talocalcaneal joint, but the calcaneocuboid relationship is abnormal, with medial subluxation of the cuboid relative to the calcaneus (short arrow). The fracture is horizontally oriented on the lateral view. There is dorsal and medial soft tissue swelling around the navicular. Minimally displaced fracture is also present at the anterior process of calcaneus (arrowhead).


Case 9-15. Navicular stress fracture. AP radiograph and axial CT image of the foot. There is a vertically oriented minimally displaced fracture through the mid aspect of the navicular bone (arrows). Fracture line extends into the talonavicular joint as well as into the naviculocuneiform joint. Stress fractures of the navicular bone are most likely due to compression forces generated by exercise, particularly running. Radiographically the fracture presents as a radiolucent line in the midportion of the navicular bone perpendicular to the talonavicular joint. It may be complete or incomplete [7].



Case 9-16. Navicular fracture from falling down stairs. AP, oblique, and lateral radiographs of the foot. There is a horizontally oriented displaced fracture through the mid aspect of the navicular bone (black arrow). The fracture extends into the talonavicular joint as well as into the naviculocuneiform joint with dorsal dislocation of the anterior fragment at the naviculocuneiform joint (white arrows).



Case 9-17. Lisfranc fracture-dislocation (homolateral type) from sledding accident. AP, oblique, and lateral radiograph of the foot. There is lateral dislocation of the first through the fifth metatarsals at the tarsometatarsal joint. The first metatarsal bone is articulating with the middle cuneiform on AP and oblique views, and the whole metatarsals are dorsally dislocated with respect to tarsals at the tarsometatarsal joint. Small avulsed fragments are noted at the metatarsal bases on the lateral view (arrows). There is severe dorsal and medial soft tissue swelling around the midfoot. The Lisfranc injury is basically dislocation of the tarsometatarsal joints. There are two basic forms of injury. The homolateral type is a dislocation of the metatarsals, usually the second through the fifth or all five, more commonly lateral than medial. The divergent type is a lateral displacement of the second through fifth metatarsals and medial displacement of the first metatarsal.



Case 9-18. Lisfranc fracture-dislocation (divergent type) from high speed motor vehicle accident. AP, oblique, and lateral radiograph of the foot demonstrate first metatarsal shaft is dislocated medially and the second through the fifth metatarsals are displaced laterally.

Case 9-19. Lisfranc fracture-dislocation. AP radiograph of the foot demonstrates widening of the joint space between the first and the second metatarsals with avulsed bony fragments. The medial border of the second metatarsal shows more than 2mm lateral displacement and step-off with respect to the medial border of the middle cuneiform (arrow). There are oblique, displaced fractures at the second and the third metatarsal necks. It has been stated that as many as 20% of these injuries have been overlooked. The findings can be subtle and occasionally are only evident on a single view [10].


Case 9-20. Shotgun injury. AP and lateral radiographs of the foot and ankle demonstrate numerous shotgun pellets (birdshot) throughout the soft tissues of the ankle and foot. There is a comminuted fracture at the distal tibia and fractures of the midfoot are likely to be present but obscured by the projectiles. Shotguns are popular worldwide; in the hands of civilians, more of these weapons exist than the rifled types of long guns. Shotgun wounds differ from those of other missiles because the volume of issue struck directly by projectiles is large owing to the fact that the pellets spread apart as they travel away from the barrel. Close-range shotgun wounds can be as destructive as those from a high velocity rifle, but longer weapon-victim ranges may produce only minimal injury. The type of shot (size and weight of pellets) used also determines the type of injury, with more serious injuries produced by the larger type of buckshot (greater than 0.14 inches in diameter) [11].

Case 9-21. Fifth metatarsal base fracture (Dancers fracture). An oblique radiograph of the foot shows a transverse, incomplete fracture at the fifth metatarsal base at the tuberosity (arrow). A dancer fracture is usually considered to be an avulsion fracture of the base of the fifth metatarsal when traction is exerted from the peroneus brevis tendon or lateral cord of plantar aponeurosis.



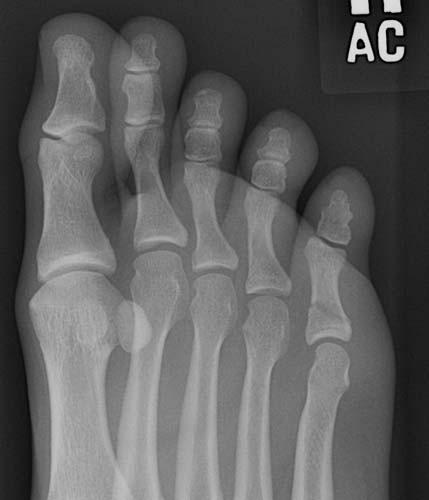
Case 9-22. Fifth metatarsal fracture of an 11-year-old boy after eversion injury. AP, oblique, and lateral radiographs of the foot of a child. There is a small transverse avulsion fracture (short arrows) at the fifth metatarsal tuberosity, next to the apophysis (long arrow). In children, the longitudinally oriented apophysis found at the lateral margin of the base of the fifth metatarsal may be mistaken for an avulsion fracture. However, apophysis is longitudinally oriented, as opposed to the transverse orientation of a fracture.



Case 9-23. Fifth metatarsal fracture (Jones fracture). Oblique, AP, and lateral radiographs of the left foot. An incomplete, transverse fracture (arrows) is noted at the proximal fifth metatarsal diaphysis. Fractures of the base of the fifth metatarsal are among the most common of all skeletal injuries of the foot. Despite their common occurrence, there has been considerable confusion in the literature regarding these injuries. Fractures of the base of the fifth metatarsal may occur proximal to the expanded tuberosity, through the expanded tuberosity, or distal to the tuberosity in the proximal diaphysis. The original description of Jones designates fractures that occur 0.75 inch (2 cm) from the metatarsal base as Jones fractures. The classic Jones fracture could be an acute fracture from a single accident or a stress fracture, or occasionally an insufficiency fracture. These fractures often undergo delayed union or even nonunion, and operative intervention may be required [7, 12].



Case 9-24. Fifth metatarsal fracture (Jones fracture). Oblique, AP, and lateral radiographs of the foot demonstrate an incomplete, transverse fracture (arrows) at the proximal fifth metatarsal shaft with some callus formation (arrowhead) indicating subacute fracture.



Case 9-26. Fifth metatarsal fracture after falling from a jump. Oblique, AP, and lateral radiographs of the foot show minimally displaced oblique fracture at the fifth distal metatarsal shaft and neck.



Case 9-27. Metatarsal shaft fracture after the patient landed hard on his foot while playing soccer. AP, oblique, and lateral radiographs of the foot. There are transverse, incomplete fractures at the second and the third metatarsal midshaft. Fractures of the shaft and neck of the metatarsal bones and phalanges are usually the result of heavy objects falling on the foot. Less commonly the phalanges may be fractured as the foot strikes furniture or other objects. These fractures are transverse, oblique, or comminuted. Rarely a longitudinal linear fracture is encountered [7].

Case 9-28. Open metatarsal fracture from motor vehicle accident. An AP radiograph of the foot demonstrates an oblique and impacted fracture of the second metatarsal neck with one shaft width lateral displacement of the distal fragment. There are also laterally displaced fractures through the bases of the third, fourth, and fifth metatarsals (arrow). Air is present throughout the soft tissues of the foot indicating open fracture.

Case 9-29. Second metatarsal stress fracture. An AP radiograph of the foot demonstrates periosteal callus formation along the medial aspect of the second metatarsal shaft (arrow) without definite fracture line. The metatarsals are the site of the most common stress fracture. It is particularly common in the military recruit population but can be encountered in any activity done in excess, such as hiking or running. The radiographic findings are not evident initially. In 7 to 10 days a transverse radiolucency or fluffy periosteal reaction appears, indicating the site of fracture [7].



Case 9-30. Multiple forefoot fracture-dislocation. Foot injury while participating in motocross. AP, oblique, and lateral radiographs of the foot. There is an avulsion fracture of the medial margin of the proximal phalanx of the great toe, at the attachment of the medial collateral ligament. The fragment is displaced relative to the remainder of the proximal phalanx, and the articular surface of the proximal phalanx is slightly subluxated in the lateral direction relative to the first metatarsal head. This combination of features suggests lateral fracture dislocation, with subsequent relocation. The medial and lateral sesamoids are abnormally separated, suggesting injury of the flexor mechanism of the great toe. The lateral sesamoid appears to be fractured. There are laterally displaced fractures of the necks of the second through fifth metatarsals, with the MTP joints still intact. The foot is highly vulnerable in motocross, and this injury suggests there was violent abduction of the forefoot.


Case 9-31. Multiple fractures, dislocations, and degloving of the toes. While wearing sandals, the patient’s foot was run over by a city bus. AP and oblique radiographs of the foot. The IP joint of the great toes is dislocated, with overlap of the proximal and distal phalanges at the joint. The second toe has sustained a transverse fracture of the proximal phalanx with one shaft width displacement. There is lateral dislocation of the DIP joint of the third toe. In addition, there is a fracture of the tip of the distal phalanx with degloving of the distal soft tissues from the remaining bones of the toe. At the fourth toe, there are fractures of the distal and middle phalanges with degloving. At the fifth toe, there is a fracture of the distal phalanx with degloving. There as been complete degloving of the fourth and fifth toes, with the soft tissues squeezed off of the bones by the bus tire as it ran over the foot.

Lateral radiograph of the foot. There is dorsal dislocation of the first proximal phalanx at the interphalangeal joint (arrowhead). Gas in the soft tissue surrounding the toes is consistent with open fractures.



Case 9-32. First metatarsophalangeal joint dislocation from motor vehicle accident. AP, oblique, and lateral radiographs of the foot. On AP view there is slight overlapping of the first metatarsophalangeal joint (arrowhead). On the oblique view, the first MTP joint appears misaligned or subluxated (short arrow). On the lateral view, there complete dislocation of the great toe at the MTP joint with dorsal displacement of the proximal phalanx relative to the first metatarsal (long arrow). There is no fracture. Dislocations of the IP and MTP joints are common. In general, the fractures, fracture-dislocations, and dislocations of the toes are quite similar those encountered in the metacarpals and phalanges of the hand [7].



Case 9-33. Fifth metatarsophalangeal joint dislocation from 30 foot fall. AP, lateral, and oblique radiographs of the foot. On AP view, there is lateral dislocation of the fifth proximal phalanx with respect to the fifth metatarsal. On lateral view, the fifth proximal phalanx is dorsally dislocated (arrow). There is no fracture. An oblique view demonstrates overlapping of the fifth metatarsophalangeal joint (arrowhead). Dorsal dislocation may be hard to detect on the oblique view.


Case 9-34. Sesamoid fracture without history of injury. AP and oblique radiographs of the great toe. There is a non-displaced transverse fracture of the lateral sesamoid of the great toe (arrow). Occasionally there is a transverse or oblique fracture of one of the sesamoid bones of the great toe, more commonly the tibial or medial sesamoid. In some cases this may actually represent a stress fracture [13-14]. Normal bipartite sesamoids are distinguished from fractures by the cortical margin of the opposing surfaces and the slightly beveled appearance at the level of the synchondrosis.


Case 9-35. Sesamoid fracture. The patient is a woman with chief complaint of pain underneath the first metatarsophalangeal joint for 3 months. Her work requires standing for 12-hour shifts, and she is an avid recreational ballroom dancer. AP and lateral radiographs of the great toe. There is a non-displaced transverse fracture of the lateral sesamoid of the great toe (arrows). A fracture may be distinguished from the more common bipartite sesamoid by the sharpness and narrowness of the fracture line and the lack of cortical margins. In addition, the fracture fragments should look as if they could fit back together perfectly, while the separate ossifications of a bipartite (or multipartite) bone would not fit together as well. Most fractures of the sesamoids of the great toe are stress injuries [13-14].


Case 9-36. Great toe (proximal phalanx) fracture. The patient landed on another player while playing basketball. AP and oblique radiographs of the foot. There is a minimally displaced oblique fracture of the first proximal phalanx extending in to the first interphalangeal joint, distally (arrow). The fracture is not clearly seen on the oblique view.



Case 9-37. Third toe (distal phalanx) fracture. The patient stubbed his toe. Lateral, AP, and oblique radiographs of the third toe. There is a subtle fracture at the dorsal margin of the base of the distal phalanx of the third toe. The minimal displacement only seen on the lateral radiograph (arrow in A). Soft tissue swelling is present around the distal interphalangeal joint.

Case 9-38. Fifth toe (proximal phalanx) fracture – oblique. An oblique radiograph of the foot demonstrates an oblique, minimally displaced fracture of the fifth proximal phalanx (arrow).

Case 9-39. Fourth and fifth toe (proximal phalanges) fractures. The patient whacked toes into a wooden banister off the staircase while she was running down stairs. AP and oblique radiographs of the foot demonstrate minimally displaced oblique fractures of the fourth and fifth proximal phalanges (arrows).


Case 9-40. Second toe (proximal phalanx) fracture. A 70-year-old female patient stumbled at home. AP and oblique radiographs of the foot demonstrate an oblique fracture through the proximal second phalanx (arrows). There is mild displacement of the fracture fragments. There is adjacent soft tissue swelling.


Case 9-41. Fourth and fifth toe (proximal phalanges) fractures after falling down from standing. AP and oblique radiographs of the foot demonstrate mildly displaced fractures of the proximal phalanges of the fourth and fifth toes (arrows).


Case 9-42. Fifth toe (proximal phalanx) fracture. The patient accidentally kicked a piece of furniture in the house while walking barefoot. AP and oblique radiographs of the foot demonstrate an oblique, minimally displaced fracture of the fifth proximal phalanx (arrow).


Case 9-43. Fifth toe (proximal phalanx) fracture. The patient dropped a speaker of the foot. AP, and oblique radiographs of the foot demonstrate non-displaced transverse fracture through the shaft of the fifth proximal phalanx (arrow). There is soft tissue swelling about the fracture site.



Case 9-44. Fifth proximal interphalangeal joint dislocation. The patient stubbed his fifth toe. AP, oblique, and lateral radiographs of the foot demonstrate dorsal dislocation of the fused fifth distal and middle phalanges at the proximal interphalangeal (PIP) joint. The fifth PIP joint is narrowed and overlapped on AP and oblique radiographs (arrows), however, there is complete dislocation on the lateral radiograph (arrow).

Case 9-45. First and second toe (distal phalanges) fractures. AP radiograph of the foot demonstrates crushed injury at the first and second distal phalanges (arrows).



Case 9-46. Forefoot amputation. AP, oblique, and lateral radiographs of the foot demonstrating crushed injury with amputation of the forefoot from the first through the fourth digits at the level of metatarsophalangeal joints. The fifth proximal phalanx shows fracture but its not amputated.

Radiograph of amputated forefoot demonstrates comminuted fractures at the amputated stumps and soft tissue injury. Unlike the hand, where the aesthetic restoration of function by replantation of amputated digits may be crucial to the rehabilitation of the patient, replantation of the toes is rarely if ever performed. The prognosis for replantation of complete great toe amputation is poor [15].

Case 9-47. Os peroneus fracture. An oblique radiograph of the foot shows avulsed and distracted fracture of the os perineum (arrow). The os peroneum is a sesamoid bone located within the peroneus longus tendon in the region of the cuboid tunnel. It is present in its fully ossified form in up to 20% of adults and is bilateral in approximately 60% of cases. A bipartite appearance is a frequent finding, occurring in approximately 30% of adults with an os peroneum. A fracture of an os peroneum can occur after trauma and may be associated with a peroneus longus tendon tear. Radiographic differentiation between a fractured os peroneum and a multipartite os peroneum can be problematic. In an acute setting, the fracture margins appear relatively non-sclerotic and the bone fragments typically fit together like pieces of a puzzle. Conversely, a rounded, smooth, sclerotic margin is consistent with multipartite os peroneum. It is conceivable that remodeling of fracture fragments over time could give the appearance of a multipartite os peroneum [16].
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


