and Sofia Gourtsoyianni2
(1)
UOC Radiologia BR, Azienda Ospedaliera Universitaria Integrata Verona, Verona, Italy
(2)
Imaging 2, Level 1, Lambeth Wing St Thomas’ Hospital, London, UK
MEN
Multiple endocrine neoplasia (MEN) syndromes are a collection of autosomal dominant syndromes characterised by the presence of multiple endocrine tumours.
Multiple endocrine neoplasia (MEN) type I, also known as Wermer syndrome, is characterised by parathyroid hyperplasia, islet cell tumours of the pancreas (most often gastrinomas, followed by glucagonomas) and pituitary adenomas.
MEN type II is associated with medullary thyroid cancer, parathyroid tumours and pheochromocytoma.
Metastases, Liver
Liver is the second most frequent metastatic site, with liver metastases being the most common form of malignant liver disease. The single best examination with lower rate of further imaging for therapy decision in case of liver metastasis detection has been shown to be EOB-DTPA MRI, compared to extracellular contrast agent MRI and triple-phase MDCT examination.
Thyroid carcinoma, carcinoid, neuroendocrine tumours, RCC and to a lesser extent pancreas, breast and colon cancer and cancer of unknown primary give hypervascular liver metastases at early dynamic phase, which then demonstrate typical washout on portal venous phase (Fig. 1).
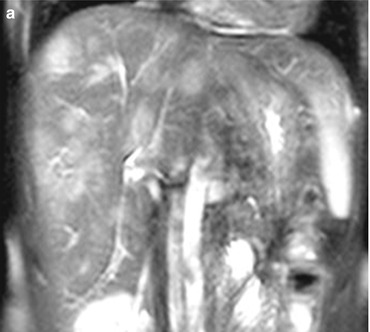
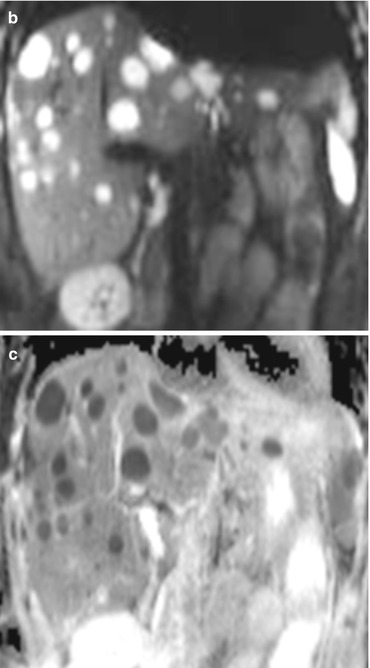
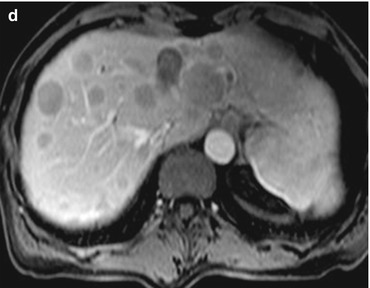
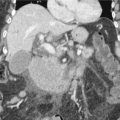
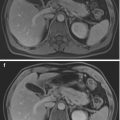
Fig. 1
Liver metastases: multiple T2-w hyperintense liver lesions are noted in both liver lobes (a) that present with restricted diffusion (high signal intensity on b 800 image b, low signal intensity on corresponding ADC map (c) and demonstrate enhancement pattern typical for liver metastases (d). The patient was found to have a small bowel carcinoid
Hypovascular liver metastases encountered predominantly in colon, lung, breast and gastric primaries are hypointense on all phases and may demonstrate perilesional enhancement in the arterial phase due to peritumoral desmoplastic reaction, presence of inflammatory cells and vascular proliferation.
Metastases, Pancreas
Pancreatic metastases are rare and account for 2–5 % of all pancreatic malignancies. The most common primaries include renal cell carcinoma, melanoma, breast cancer, lung cancer, gastric cancer and colorectal carcinoma.
Most pancreatic metastases are asymptomatic and detected incidentally at imaging or autopsy. Larger lesions, especially if in the head of the pancreas, may cause jaundice, pancreatic insufficiency, duodenal/gastric obstruction and GI bleeding.
Metastases can involve any portion of the organ and present as a localised mass in most cases (50–75 %). Less common are a diffuse involvement of the pancreas (5–45 %) and the presence of multiple nodules (5–15 %).
Metastases are usually small well-circumscribed masses, iso- to hypodense to the normal parenchyma on non-contrast scans. Calcifications are rare. Post-contrast enhancement resembles that of the primary tumour and is usually homogeneous in smaller lesions and peripheral in larger lesions, presumably due to central necrosis (Fig. 2).

Fig. 2
Pancreatic metastases: arterial phase CT shows multiple small hypervascular pancreatic lesions, consistent with metastases in a patient with history of renal cell carcinoma
Metastases in the head of the pancreas commonly cause pancreatic ductal obstruction and may be associated with common bile duct obstruction.
Mirizzi Syndrome
The Mirizzi syndrome refers to obstruction of the common hepatic duct caused by an extrinsic compression from an impacted stone in the cystic duct or Hartmann’s pouch of the gallbladder. It was initially described by the Argentinian surgeon Pablo Luis Mirizzi in 1948.
It is a functional hepatic syndrome but can often present with biliary duct dilatation and can mimic other hepatobiliary pathology such as cholangiocarcinoma.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


