This article presents current magnetic resonance imaging techniques for the diagnosis of biliary tumors. It emphasizes the need for a comprehensive protocol, combining imaging sequences of the liver parenchyma and soft tissues with magnetic resonance cholangiopancreatography and magnetic resonance angiography to detect and stage biliary malignancies. Imaging characteristics that may indicate a specific diagnosis are discussed. The potential role of diffusion-weighted imaging in diagnosing the cause of biliary obstruction and detecting unsuspected nodal disease and peritoneal seeding is emphasized and illustrated.
Bile duct imaging
Magnetic resonance (MR) imaging has been accepted as a major noninvasive diagnostic modality for investigating the bile ducts. MR imaging with MR cholangiopancreatography (MRCP) may be used as a replacement for diagnostic endoscopic retrograde cholangiopancreatography (ERCP) in many indications and has gained acceptance by gastroenterologists, surgeons, and general practitioners because of its high success rate, and because of the ability to project a virtual cholangiogram image display.
MR imaging assessment of bile duct morphology may be combined with evaluation of the liver parenchyma, adjacent soft tissues, and vascular network for biliary tumor detection, staging, and surgical planning. Rapid T1- and T2-weighted sequences with high spatial resolution are commonly available as a result of the technological advances in MR imaging. Furthermore, the detection of hepatobiliary malignancy through the use of nonconventional MR imaging techniques has become more readily accessible because of the advances in functional MR techniques in the abdomen, such as diffusion-weighted imaging (DWI) with high b values and acceptable signal-to-noise ratio. This article discusses the current MR imaging techniques for the diagnosis of biliary tumors. Emphasis is placed on the importance of a comprehensive protocol that includes: T2-weighted imaging and MRCP, gadolinium-enhanced T1-weighted imaging, and DWI. Imaging characteristics that may indicate a specific diagnosis of biliary tumor are described.
MR imaging technique
General Considerations
Comprehensive MR imaging of biliary tumors should:
- 1.
Show the size and location of a primary lesion and assess the longitudinal and radial extent of bile duct involvement
- 2.
Enable the characterization of a biliary stenosis
- 3.
Show involvement of the hepatic artery (main and lobar branches) and portal vein (main and lobar branches) with the tumor, for the purpose of surgical planning
- 4.
Depict the presence and extent of liver invasion and lobar atrophy or hypertrophy
- 5.
Enable the detection of regional lymph nodes and metastases.
To achieve such a level of assessment, MR imaging should be performed at high field strength using multichannel, phased-array coils, parallel imaging technology, and ideally before any biliary drainage procedure. Such an approach allows high-resolution images to be obtained with substantially reduced acquisition times.
The major advantage of parallel imaging is a reduction in acquisition time. Parallel imaging in conjunction with turbo spin-echo (TSE) T2-weighted sequences, allows shortening of the echo train length without loss of spatial resolution, and consequently decreases signal decay and reduces image blurring. The use of parallel imaging to shortening the acquisition time is also beneficial in gradient-echo (GRE) T1-weighted imaging, because it permits image acquisition within a breath hold. A further advantage of parallel imaging is the reduction in geometric distortion and image ghosting when it is used in combination with modern fat suppression schemes, which is particularly helpful for DWI.
DWI of the liver is of particular interest as a means of exploring new contrast mechanisms in which signal intensity reflects the degree of restriction of microscopic water movements in tissues and is correlated to tissue cellularity, the integrity of cell membranes, and the amount of tissue fibrosis. DWI is therefore a sensitive sequence for the detection of tumors and inflammation and may be beneficial in the assessment of patients with contraindications for gadolinium administration. In addition, DWI has the potential advantage of performing quantitative data analysis through the generation of apparent diffusion coefficient (ADC) maps, which could contribute to objective disease assessment and monitoring of response to therapy. With modern MR scanners a complete assessment of the biliary system and its surrounding tissues can be performed in approximately 30 minutes.
Practical Setup
Patients are required to fast for 4 to 6 hours before the examination, to permit gallbladder distension and promote gastric emptying. The presence of a large amount of fluid in the bowel may interfere with image interpretation because of the visualization of overlapping bowel loops. Strategies to overcome the potential obscuring of biliary structures by fluid in bowel include the administration of a T2-negative oral contrast agent (iron oxide particles, or pineapple juice or 1 mL of gadolinium mixed with 50 mL of water). However, duodenal distension may be desirable when detailed visualization of the duodenal papilla and the confluence of bile and pancreatic ducts is required. In such selected patients duodenal distension may be achieved with administration of secretin, which stimulates pancreatic exocrine fluid and to a lesser extent secretion of bile duct fluid.
The 4 principle sequences used for imaging the hepatobiliary system are:
- 1.
TSE T2-weighted imaging
- 2.
Thick-slab MRCP cholangiogram
- 3.
DWI
- 4.
Pre- and postgadolinium-enhanced volumetric fat-suppressed GRE T1-weighted imaging.
Sequences
- 1.
T2-weighted sequence: Thin section T2-weighted images are acquired in the axial and coronal planes using a single-shot TSE sequence during free breathing with respiratory triggering or a navigator echo, to minimize the need for patient cooperation. The field of view should include the whole liver, the pancreas, and the duodenum, with a typical section thickness of 4 to 5 mm. To preserve the delineation of surrounding anatomy, fat suppression is not routinely applied. The T2-weighted images provide good contrast between lesions with high water content and the adjacent liver and soft tissues and depict the bile ducts and the pancreatic ducts in cross section. The T2-weighted images are also used as a guide for thick-slab MRCP acquisition ( Table 1 and Fig. 1 ).
Table 1Related posts:
 MR Imaging of Benign Focal Liver Lesions
MR Imaging of Hepatocellular Carcinoma
Diffusion-Weighted MRI and Liver Metastases
MR Imaging of Benign Focal Liver Lesions
MR Imaging of Hepatocellular Carcinoma
Diffusion-Weighted MRI and Liver Metastases
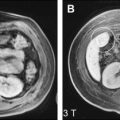 Imaging at Higher Magnetic Fields: 3 T Versus 1.5 T
Imaging at Higher Magnetic Fields: 3 T Versus 1.5 T
 Magnetic Resonance Imaging of the Liver: Sequence Optimization and Artifacts
Magnetic Resonance Imaging of the Liver: Sequence Optimization and Artifacts
 Functional Magnetic Resonance Imaging of the Liver: Parametric Assessments Beyond Morphology
Functional Magnetic Resonance Imaging of the Liver: Parametric Assessments Beyond Morphology

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


