Magnetic Resonance Imaging of the Shoulder
Clyde A. Helms
MR of the shoulder is well accepted for its diagnostic utility for abnormalities of the rotator cuff and the glenoid labrum. It has been shown to have a high degree of accuracy (1,2,3,4). MR of the shoulder can be performed following instillation of gadolinium and saline or without arthrography, with some controversy as to which technique is superior.
Anatomy
The rotator cuff is composed of the tendons of four muscles that converge on the greater and lesser tuberosities of the humerus: the supraspinatus, infraspinatus, subscapularis, and teres minor (Fig. 48.1). Of these, the supraspinatus most commonly causes clinically significant problems and is the one that is most commonly surgically treated. The supraspinatus tendon lies just superior to the scapula and inferior to the acromioclavicular (AC) joint and acromion. It inserts onto the greater tuberosity of the humerus. Two to three centimeters proximal to its insertion is a section of the tendon called the “critical zone.” This area is reported to have decreased vascularity and is therefore less likely to heal following trauma. The critical zone of the supraspinatus tendon is a common location for rotator cuff tears. Most cuff tears, however, begin at the bone/tendon interface on the greater tuberosity.
The glenoid labrum is a fibrocartilaginous ring that surrounds the periphery of the bony glenoid of the scapula. It serves as an attachment site for the capsule and broadens the base of the glenohumeral joint to allow increased stability. Tears or detachments of the glenoid labrum most commonly occur from, and result in, dislocations or instability of the humerus.
Rotator Cuff
The rotator cuff commonly suffers from what has been termed “impingement syndrome.” Impingement of the supraspinatus tendon occurs from abduction of the humerus, which allows the tendon to be impinged between the anterior acromion and the greater tuberosity. The tendon can also be impinged by the undersurface of the AC joint if downward-pointing osteophytes or a thickened capsule is present. Other theories exist for rotator cuff disease, including natural degeneration from aging and a predisposition for the cuff to undergo degeneration due to decreased blood supply. Most investigators agree that whatever the cause, the natural course of impingement syndrome or cuff degeneration is a complete, or full-thickness, tear of the rotator cuff.
The rotator cuff is best seen on oblique coronal images that are aligned parallel to the supraspinatus muscle (Fig. 48.2) and on the oblique sagittal images (Fig. 48.3). Both T1-weighted (or proton density) and T2-weighted sequences are typically performed, although little diagnostic information is present on the T1WIs and they are not obtained by many radiologists. Multiple acceptable variations of imaging sequences are available to demonstrate the normal and abnormal structures that can be seen. A fat-suppressed fast spin-echo (FSE) T2-weighted oblique coronal is gaining popularity as the primary sequence for imaging the rotator cuff in many imaging centers. The slice thickness should be no greater than 5 mm, and 3 mm is preferable. As with most joint imaging, a small field of view (16 to 20 cm) is recommended. A dedicated shoulder coil or a surface coil placed anteriorly over the shoulder is necessary.
When a joint effusion is present, the intra-articular structures, such as the labrum, biceps, and articular surface of the cuff, are more easily evaluated. Therefore, many feel an MR following an arthrogram is superior to a non-arthrogram MR. An MR arthrogram is typically performed by injecting 10 to 15 mL of a saline/gadolinium mixture and then obtaining T1WI with fat suppression, in addition to T2WI in multiple planes. This can be a time-consuming exam; hence, some centers have begun injecting 10 to 15 mL of saline for joint distension and omitting the gadolinium (5). This means the fat-suppressed T1WI can be eliminated, which saves considerable imaging time. High-quality T2WIs with fat suppression are very close to the quality of images obtained with T1 weighting (they suffer minimally from a decreased signal-to-noise ratio).
In examining the rotator cuff, the most anterior oblique coronal images will show the supraspinatus tendon. A useful landmark for noting the anterior portion of the supraspinatus tendon is the bicipital groove, which has the anterior most fibers of the supraspinatus immediately lateral to the groove. This is where most cuff tears begin and can be overlooked if the patient’s shoulder is internally rotated, which is common (6) (Fig. 48.4).
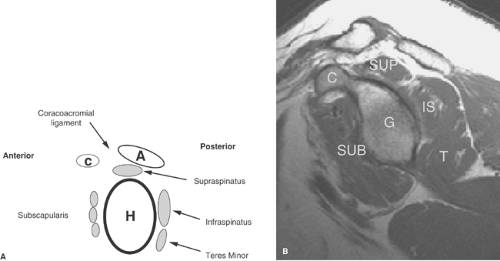 Figure 48.1. Normal Shoulder Anatomy. A. This drawing shows the rotator cuff muscles in a sagittal plane (anterior is on the left). C, coracoid; A, acromion; H, humeral head. B. This sagittal T1WI through the glenoid shows the normal cuff musculature (SUB, subscapularis; SUP, supraspinatus; IS, infraspinatus, T, teres minor, C, coracoid process, G, glenoid). |
The normal supraspinatus tendon is said to be uniformly low in signal on all pulse sequences. Unfortunately, this is not always the case. In fact, it often has some intermediate-to-high signal in the tendon, which causes much confusion. If the signal in the tendon gets brighter on the T2WIs, it is abnormal
and represents either tendinitis (most investigators prefer the term “tendinosis” or “tendinopathy” over tendinitis, as no inflammatory cells are found histologically) or a partial tear. A partial tear can be diagnosed by noting thinning of the tendon itself (Fig. 48.5).
and represents either tendinitis (most investigators prefer the term “tendinosis” or “tendinopathy” over tendinitis, as no inflammatory cells are found histologically) or a partial tear. A partial tear can be diagnosed by noting thinning of the tendon itself (Fig. 48.5).
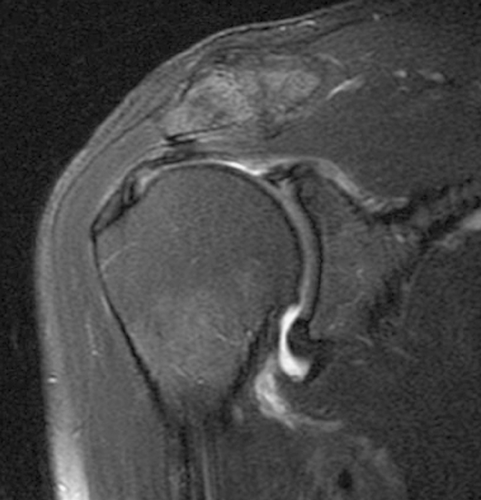 Figure 48.2. Oblique Coronal Image of Normal Rotator Cuff. This oblique coronal image fast spin-echo T2WI with fat suppression through the supraspinatus shows a normal supraspinatus with a broad footprint where the tendon inserts onto the greater tuberosity. |
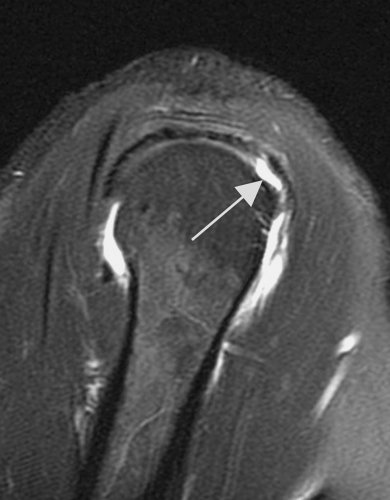 Figure 48.3. Oblique Sagittal Image of a Torn Rotator Cuff. An oblique coronal image fast spin-echo T2WI with fat suppression shows the rotator cuff inserting onto the greater tuberosity in a normal fashion except at the far anterior portion (arrow). This indicates a partial tear of the articular surface fibers of the cuff. |
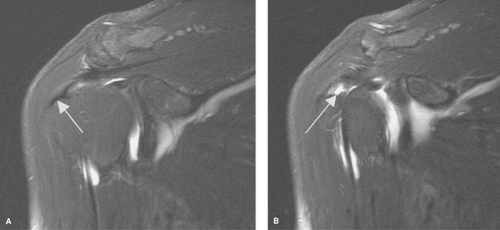 Figure 48.4. Internal Rotation Hiding Partial Tear of the Supraspinatus Tendon. A. An oblique coronal fast spin-echo T2WI with fat suppression shows an apparent normal supraspinatus inserting onto the greater tuberosity (arrow). B. One slice more anteriorly the bicipital groove can be identified with the fibers of the supraspinatus just lateral to the groove lifted off of the greater tuberosity (arrow). This is a partial tear of the rotator cuff at its anterior most portion. |
Myxoid and fibrillar degeneration of the supraspinatus tendon are commonly found in autopsy specimens in older patients. The majority of asymptomatic shoulders in patients over the age of 50 are believed to have some tendon degeneration in the supraspinatus; this has been termed “tendinopathy.” This is seen as high signal in the critical zone on T1WIs that does not increase with T2 weighting (7). Many reserve the term myxoid degeneration for those cuffs that display intermediate signal as well as some thickening (Fig. 48.6).
Myxoid degeneration is felt by many surgeons to be more significant than anatomic impingement as a source of cuff pathology (8). Rather than decompressing the coracoacromial arch by removing bony structures and the coracoacromial ligament, which might be sources of impingement, these surgeons resect the areas of myxoid degeneration in the cuff tendons.
Tendon degeneration (tendinopathy) can be seen in asymptomatic shoulders of all ages; hence, it needs to be correlated with the clinical picture. If the signal gets brighter on T2WIs, it must be considered pathologic—either tendinitis or a partial tear.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


