Fig. 4.1
Sequential images of the opening and closing cycle of the jugular and vertebral valve system (from a to e) as dynamically shown also in Movie 4.1. First of all, it can be noted that the IJV valve leaflets have a different length and mobility, which comes clearly across from the movie, especially regarding the upper leaflet compared to the lower one. It can also be seen that they have a dissimilar mobility as compared to the leaflets of the vertebral valve, which closes up completely by the overlapping of the leaflets (c and d), whereas the jugular valve leaflets do not seem to overlap in any phase of the cycle
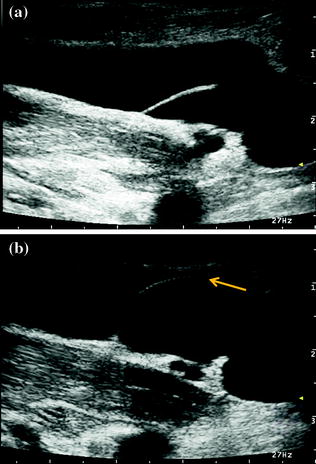
Fig. 4.2
Freeze-frame of J1 IJV during spontaneous breathing (a) and during Valsalva maneuver straining (b) in the same subject of the previous figure (see also Movie 4.2). At rest, as it clearly comes across also in the previous figure and movie, the closing of the leaflets is only occasional and not continuous with the posterior leaflet hypomobility. On the other hand, during the Valsalva maneuver, there is a perfect closure of the leaflets (arrow) with valve system continence. The morphological hypomobility of the lower leaflet of the IJV valve, in this case, seems to be a morphological alteration which does not seem to affect the local hemodynamics
Fig. 4.3
Freeze-frame of J1 IJV during spontaneous breathing (a) and during Valsalva maneuver straining (b) in color-mode in the same subject of the previous figure (see also Movie 4.3). During spontaneous breathing, there is the confirmation of the hypomotility of the lower leaflet, which also causes a kind of preferential flow channelling along the leaflet itself, together with the laminar flow spontaneously directed toward the upper leaflet. In such a situation, the Doppler waveform will show a bidirectional flow signal, due to the mingling of two different directions of the laminar flow. However, during the Valsalva maneuver the closure of the leaflets is complete without incontinence
Fig. 4.5
J1 IJV longitudinal scan with two different insonation approaches: lateral (a), see also Movie 4.4), and anterior (b), see also Movie 4.5). More specifically, it is to be noted how the redundancy of the leaflets stands out in both approaches. However, if only the second approach were to be used, in this case, there would be the risk of defining the leaflets as markedly hypomobile, almost like a septum, which actually is not true
Fig. 4.6
J1 IJV color-mode longitudinal scan, with anterior approach (same subject of Fig. 4.5). As substantiation of what pointed out about the former figure, it can be noted the flow patency of the valve system (see also Movie 4.6)
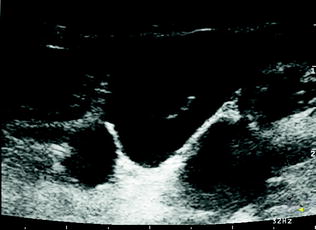
Fig. 4.8
J1 IJV color-mode longitudinal scan and corresponding Doppler waveform. Here, it is shown an example of valve incontinence caused by the Valsalva maneuver (the beginning and the end of the reflux are marked by red arrows) with a definitely significant duration (>2.5 s)
Fig. 4.9
J1 IJV color-mode longitudinal scan and corresponding Doppler waveform. Here you can see another example of valve incontinence caused by the Valsalva maneuver (the beginning and the end of the reflux are marked by red arrows) with a surely noteworthy duration (>1 s)
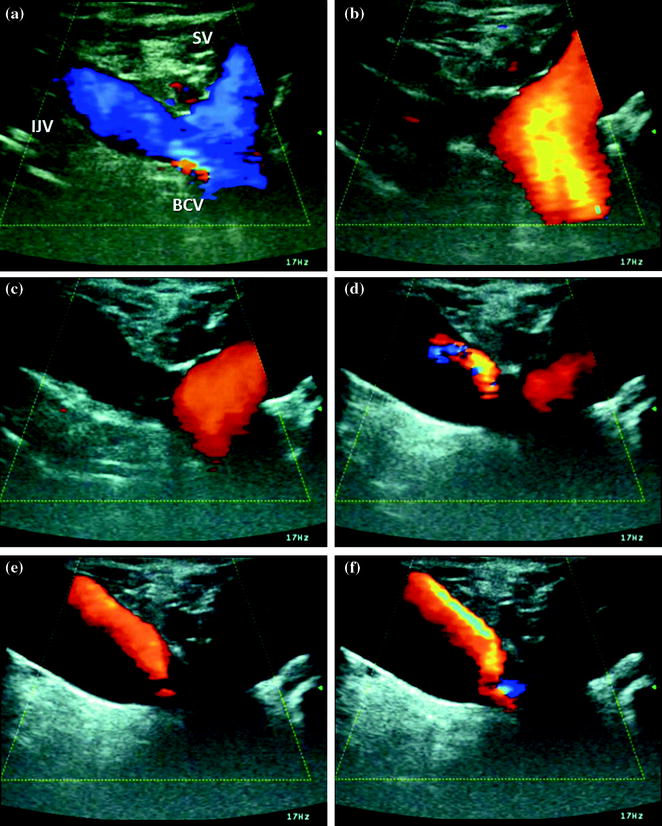
Fig. 4.10
Left IJV, subclavian access at the confluence of the SV into the BCV, color mode. Subsequent stages during the Valsalva maneuver (Movie 4.8): a Pre-Valsalva inspiration, with flow in orthograde direction in IJV, SV, and BCV. b Initial straining phase with reflux jet on the SV and absence of flow on the IJV. c Intermediate straining phase, with diminishing of the reflux jet on the SV (still absence of flux in the IJV). d At the end of the reflux jet on the SV, initial appearance of reflux jet and aliasing on the IJV. e Absence of flow on SV and extension of jet on the IJV. f Reflux jet clearly still on IJV
Fig. 4.11
B-mode J1 IJV longitudinal scan. IJV stenosis at the valve level. In the upper part of the picture (a), ultrasound image (see also Movie 4.9) that shows the fixity and distortion of the valve leaflets. In the lower part of the picture (b), the corresponding MR image that highlights the malformation with the stenosis at the jugular valve system level
Fig. 4.12
Longitudinal scan of IJV, color mode. IJV stenosis at the valve level. In this freeze-frame image with decreasing PRF, the block of flow above the valve level is showed in color mode and the marked hypomobility of valve leaflets is well evident in the B-mode movie both at rest and with a short closure during Valsalva maneuver (see Movies 4.10, 4.11). Color-mode images and the corresponding movies: PRF decreases from 2.0 kHz to 1.5, 1.3, 1.0, 0.75, 0.5 kHz. Figure 4.12 shows the same situation illustrated in Fig. 4.11, but in color mode and zoomed on the IJV valve region. In particular, note the effect of the progressive decrease in PRF value, with equal frequency in color mode. The color signal visualization within the IJV lumen occurs only with PRF of 500 Hz, which confirms the almost complete absence of flow caused by the valve system malformation
Fig. 4.13
IJV stenosis at the valve level in color mode with the Doppler waveform sampling. In figure a, the waveform in normal breathing conditions is shown; in figure b, the waveform during Valsalva maneuver marks a significant IJV valve incontinence. The valve stenosis seems a very small central hole through which the blood flow moves to and fro depending on the pressure gradient
Fig. 4.14
J2 IJV segment in the same patient of the previous figures. The upstream blood flow waveform shows a phasic ≪systolic≫ flow depending on the pressure gradient, with very low velocity. The corresponding B-mode dynamic status is a spontaneous moving echo-contrast (Movie 4.12), persisting also in color mode (Movie 4.13)
Fig. 4.15
J1 IJV of the same patient of the previous figures in M-mode (longitudinal scanning plane) at two levels of valve leaflet position. The M-line trace shows a marked hypomobility of both leaflets that remain open (asterisk)
Fig. 4.16
J2 IJV segment of the same patient of the previous figures in M-mode (longitudinal scanning plane, normal breathing). A very low movement range of the wall is evident
Fig. 4.17
Transverse scan of J2 IJV segment with afferent thyroid branch, during the inspiratory phase. Note how the dynamic characteristics of the afferent branch are evident and easy to study during the respiratory cycle
Fig. 4.18
Transverse scan of J2 IJV segment with afferent thyroid branch, during the Valsalva maneuver. Note the inversion of the flow direction in the afferent branch (a), whose Doppler waveform is illustrated in (b) (see also Movie 4.14)
Fig. 4.19
J1 IJV longitudinal scan in a condition of venous hypoplasia. Note the Doppler waveform with the flow direction shift during normal breathing. This situation very probably indicates an incomplete valve incontinence already in basal conditions with the flow direction substantially produced by the pressure gradient without significant obstacles. As to the IJV caliber evaluation, see also Movies 4.15, 4.16
Fig. 4.20
Color-mode, J1 IJV longitudinal scan in the hypoplastic vein. In this situation, the performing of the Valsalva maneuver causes a temporary, although not significant, increase in the duration of the jet reflux
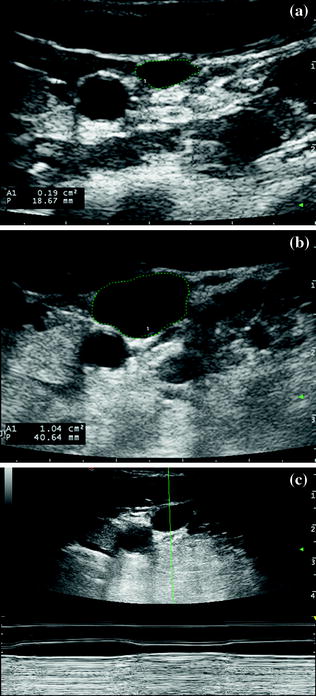
Fig. 4.21




J2 IJV, hypoplastic vein, the same subject of the former figure. In picture a, the J2 IJV CSA can be evaluated. It is decidedly reduced as expected, but it is consistent with what is described in the literature, regarding the IJV size asymmetry between one side and the other. As a comparison, in picture b, the contralateral J2 IJV area has been marked. Picture c, in M-mode, transverse access, as in Movie 4.17, a wide range of the vein caliber, connected with the respiratory cycle, is highlighted
Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
