Medial Head of Gastrocnemius Muscle Tear
Kelly L. Hastings
Daniel B. Nissman
CLINICAL HISTORY
36-year-old male with acute onset calf pain while playing tennis.
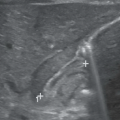
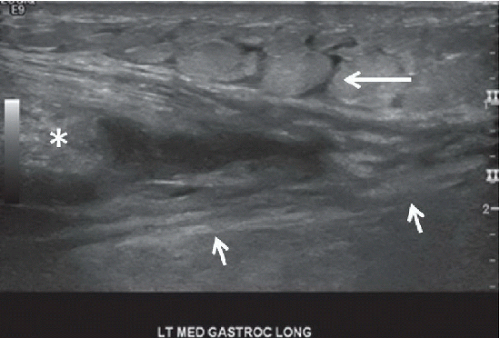 FIGURE 94A |
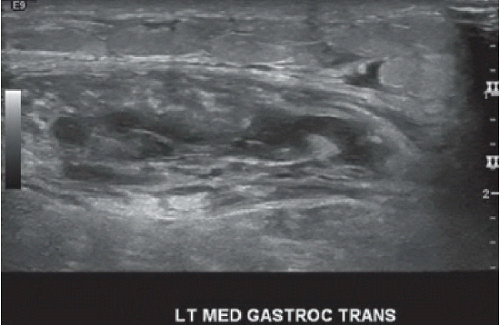 FIGURE 94B |
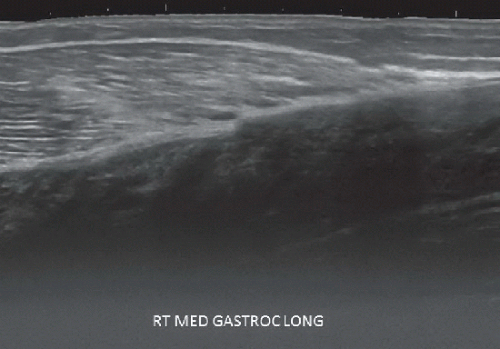 FIGURE 94C |
FINDINGS
Long/sagittal (Fig. 94A) and short/transverse (Fig. 94B) axis gray-scale sonographic images of the left medial head of gastrocnemius demonstrate a moderate- to large-sized near-triangular-shaped hypoechoic defect at the distal myotendinous junction. The heterogeneity seen on the short-axis image is consistent with a hematoma. Intact fibers are seen on the left side of the image. The asterisk indicates the retracted portion of the muscle. The short arrows point to the Achilles tendon/myotendinous junction that separates the gastrocnemius (superficial) from the soleus (deep). Interdigitating free fluid within the subcutaneous tissues (long arrow) consistent with edema is present. Long-axis view of the contralateral leg (Fig. 94C) shows the myofibrils making contact with the myotendinous junction. Note how the more distal (right side of image) fibrillar pattern appears smudged and more hyperechoic than the more proximal (left side of image) fibrillar pattern.
DIFFERENTIAL DIAGNOSIS
Medial head of gastrocnemius muscle tear, plantaris rupture, proximal Achilles tendon tear, ruptured popliteal cyst, intramuscular abscess, deep vein thrombosis.
DIAGNOSIS
Large left medial head of gastrocnemius partial tear (Figs. 94A and 94B), low-grade right medial head of gastrocnemius strain (Fig. 94C).
DISCUSSION
The gastrocnemius muscle is located in the superficial posterior compartment of the leg and predominantly provides plantar flexion at the ankle. There are two heads of the gastrocnemius, medial and lateral, which originate at the femoral condyles and unite to form the Achilles tendon along with the soleus. The gastrocnemius crosses the knee, ankle, and subtalar joints before inserting on the calcaneus. The gastrocnemius is thought to be more susceptible to injury compared with other leg muscles because of crossing the knee and ankle joints; nearly all calf muscle strain injuries involve the medial head. The medial head of gastrocnemius is larger than the lateral head and contains proportionally more “fast twitch” muscle fibers. The increased number of fast twitch fibers correlates with the medial head’s importance in running and jumping activities.1 Hyperextension of the knee in conjunction with forced dorsiflexion causes increased strain at the myotendinous junction relative to a muscle crossing only a single joint (e.g., the soleus) because of the large amount of stretch in this position. Muscle strain injuries typically occur during eccentric contraction where the muscle is contracting while lengthening; strain injuries occur only when muscle fibers are longer than the resting muscle length, which is more likely to occur with muscles crossing two joints.1 Although muscles with increased proportion of fast twitch fibers are more frequently injured and while it seems plausible that the ability to rapidly produce a contraction can exceed the strain limit of the muscle especially during an eccentric contraction, this has not been proven. Tears of the medial head of the gastrocnemius are usually sports-related injuries, commonly affecting middle-aged persons and sometimes referred to as “tennis leg,” given its association with tennis and other racquet sports. The severity of the strain injury can range from microscopic tears to complete dissociation of the myotendinous junction and nearly always occurs at the distal myotendinous junction. Onset of pain and swelling in the calf is immediate. Ecchymosis may be present.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


