Medium vestibular schwannoma without hearing deficit – upfront radiosurgery
SKULL BASE REGION
Cerebellopontine angle/internal auditory canal
HISTOPATHOLOGY
N/A
PRIOR SURGICAL RESECTION
No
PERTINENT LABORATORY FINDINGS
Pretreatment audiogram: Class A hearing bilaterally with word recognition scores at 100% in both ears
Case description
The patient presented at 40 years of age after sustaining a concussion while playing hockey. He developed persistent headaches and feelings of being “dizzy,” which prompted a magnetic resonance imaging (MRI) scan of the brain without contrast, followed by a postgadolinium MRI after an abnormality was noted on the initial images ( Figure 8.36.1 ). There was a contrast-enhancing lesion in the left internal auditory canal (IAC) extending into the cerebellopontine angle (CPA) consistent with a vestibular schwannoma (VS). He denied unilateral hearing loss or tinnitus, facial numbness, hemifacial spasm, or facial weakness. He had no history of vertigo and only reported a feeling of disequilibrium following his head injury. His neurologic examination was normal. His audiogram showed excellent symmetrical hearing in both ears ( Figure 8.36.2 ). His past medical history was unremarkable. He was counseled regarding the management options—observation, microsurgery, and radiosurgery—and chose to proceed with single-fraction stereotactic radiosurgery (SRS) ( Figure 8.36.3 ).
Radiosurgery Machine
Gamma Knife – Perfexion
Radiosurgery Dose (Gy)
12 at the 50% isodose line, maximum 24 Gy
8 isocenters to cover a volume of 2.3 cm
Number of Fractions
1
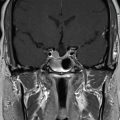
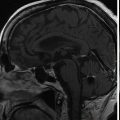
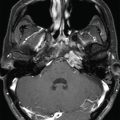
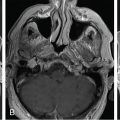
Figure 8.36.1.
Preradiosurgery MRI demonstrated a 1.3-cm, left-sided, contrast-enhancing mass centered in the cerebellopontine angle extending into the internal auditory canal and consistent with vestibular schwannoma (VS).
Figure 8.36.2.
Preradiosurgery audiogram of the left ear demonstrated normal hearing.
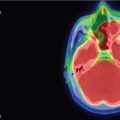
Figure 8.36.3.
A. Segmental images from MRI performed with the stereotactic headframe in place on the day of treatment showing the radiosurgical plan, including the 12-Gy (yellow) and 4-Gy (green) treatment volumes. B, C. CT-MR fusion and MR studies showing the 12-Gy treatment volume (yellow) as well as the adjacent cochlea (purple).
Critical Structure
Dose Tolerance
Cochlea
Highly controversial, recommend mean <4 Gy
Facial nerve
Single fraction doses <13 Gy appear to be very safe
Brainstem
Very dependent on volume of brainstem irradiated
Most cerebellopontine angle tumors can be safely treated with marginal doses ≤16 Gy
Side Effects/Complications
Frequency
Ipsilateral hearing loss
∼50% at 5 years and up to 75% at 10 years after stereotactic radiosurgery
Facial weakness or hemifacial spasm
1%–3% , ,
Trigeminal neuropathy
5%–10%, highest with larger tumors
Hydrocephalus
<3%, age and dose >13 Gy are risk factors
Malignant degeneration
<0.2% ,
Success Rate/Control Rate
Frequency
Unselected, all cases
>92%
Tumors growing >2.5 mm/year
69%
Larger tumors (>10 cc)
85%
Patient outcome
The patient reported no new symptoms or concerns in the first year following radiosurgery. An early postradiosurgery MRI completed 3 months after treatment showed a volumetric increase in the tumor size with associated loss of central enhancement ( Figure 8.36.4 ). Audiology again demonstrated stable and intact left-sided hearing (see Figure 8.36.4 ). Over the subsequent 8 years, serial MRIs showed a marked reduction in the tumor volume, which had largely receded to the confines of the IAC ( Figure 8.36.5 ). He also noted a slight subjective decline in hearing in the treated ear, but still uses that ear to talk on the telephone (see Figure 8.36.5 ). He has had no facial numbness, weakness, or hemifacial spasm, and no disequilibrium.
Only gold members can continue reading. Log In or Register to continue





 Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
 Null cell – delayed postoperative radiosurgery for growing perioptic residual
Null cell – delayed postoperative radiosurgery for growing perioptic residual
 Suprasellar non-small cell lung carcinoma metastasis – upfront radiosurgery
Suprasellar non-small cell lung carcinoma metastasis – upfront radiosurgery
 Chondrosarcoma – definitive radiosurgery after subtotal resections
Chondrosarcoma – definitive radiosurgery after subtotal resections
 Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
 Capillary hemangioma – postoperative radiosurgery for residual tumor
Capillary hemangioma – postoperative radiosurgery for residual tumor



