Metastatic Melanoma
Michael P. Federle, MD, FACR
Amir A. Borhani, MD
Key Facts
Terminology
Spectrum of metastatic lesions originating from known or occult malignant melanoma
Imaging
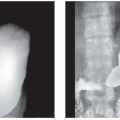
Multiple “bull’s-eye” lesions of variable size in GI tract of patient with history of skin lesion
Multiple hypervascular hepatic lesions with variable size in patient with history of melanoma
Most common sites of metastases are skin, lymph node (75%), lung (70%), liver (58%), CNS (54%), GI tract (40%)
Most common primary sites associated with abdominal metastases are head and neck, eye
Ocular melanoma has extremely high occurrence of liver metastases
Lesions are typically multiple and well circumscribed
“Bull’s-eye” or “target” lesion (secondary to central ulceration)
Top Differential Diagnoses
Leukemia and lymphoma
Hepatic metastases and lymphoma
Intestinal intramural benign tumor
Small bowel carcinoma
Kaposi sarcoma
Clinical Issues
Risk increases with age
3rd most common cancer in young adults
60% of patients with metastatic melanoma have metastases in abdomen and pelvis
Rate of metastasis correlates with depth of primary tumor into dermis
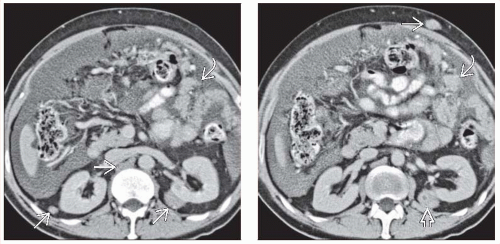 (Left) Axial CECT in a middle-aged man with cutaneous melanoma and a distended abdomen shows massive, malignant ascites due to peritoneal metastases  . Also noted are metastases to the perirenal space bilaterally . Also noted are metastases to the perirenal space bilaterally  . (Right) Axial CECT in the same patient shows additional metastases to the peritoneum . (Right) Axial CECT in the same patient shows additional metastases to the peritoneum  , abdominal wall , abdominal wall  , lymph nodes, and perirenal space , lymph nodes, and perirenal space  . “Unusual” sites of metastases are typical in patients with melanoma. . “Unusual” sites of metastases are typical in patients with melanoma. |
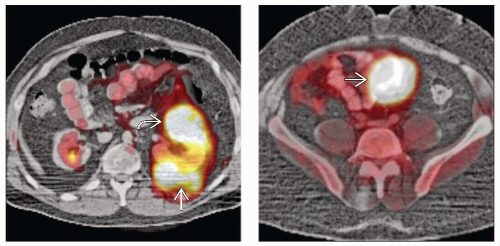 (Left) Axial PET/CT shows FDG-avid metastases in the kidney  and perirenal space and perirenal space  . (Right) Axial PET/CT in the same patient shows an additional lesion in the bowel . (Right) Axial PET/CT in the same patient shows an additional lesion in the bowel  . Despite the large size of the metastasis, there was no bowel obstruction. . Despite the large size of the metastasis, there was no bowel obstruction. |
TERMINOLOGY
Definitions
Spectrum of metastatic lesions originating from known or occult malignant melanoma
IMAGING
General Features
Best diagnostic clue
Multiple “bull’s-eye” lesions of variable size in GI tract of patient with history of melanoma
Location
Most common sites of metastases: Skin, lymph nodes (75%), lung (70%), liver (58%), CNS (54%), GI tract (40%)
Most common involved sites in abdominal cavity include liver and small bowel
Morphology
Typically multiple, in any site of body
Well-circumscribed, spherical or oval
Nodule, plaque, polypoid mass
“Bull’s-eye” or “target” lesion (central ulceration)
Imaging Recommendations
Best imaging tool
CECT, PET/CT best for total body screening
Sensitivity and specificity are ↑ by simultaneous interpretation of diagnostic quality CT
Melanoma may not be FDG avid or may be misinterpreted as normal bowel or kidney on PET
Protocol advice
Triphasic CECT
Hepatic metastases may not be visualized on monophasic CECT
86% of hepatic lesions are detected on portal venous phase as hypodense lesions
CT Findings
LiverRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree