Metastatic Tumors to the Central Nervous System
Overview
The incidence of metastatic tumors to the central nervous system (CNS) is rising in part due to advances in therapy that result in longer survival of patients with systemic cancer. Despite the development of effective immunotherapy and molecularly targeted therapies, metastatic tumors to the CNS can cause considerable morbidity and mortality in patients. Metastatic tumors to the CNS can be subdivided into five types based on the location—intraparenchymal, leptomeningeal, dural, intraventricular, and osseous compartment. Hematogenous spread is considered the most common route of entry into the CNS by metastatic tumors. Leptomeningeal carcinomatosis is poorly understood in terms of pathogenesis and mechanism of spread and remains one of the most difficult forms of metastatic tumors to treat.
Central Nervous System Metastatic Tumors
Definition: Central nervous system (CNS) metastatic tumor is a cancer that has spread from the primary (original systemic) site of the tumor to the CNS via hematogenous spread or direct extension.
Epidemiology: CNS metastases are the most common CNS neoplasms in adults but account for less than 2% of all tumors in the pediatric age group. Up to 30% of adults and 10% of children with cancer develop CNS metastases during the course of lifetime. The overall incidence of CNS metastatic tumors is increasing due to two main factors: (1) longer life expectancy of systemic cancer patients due to improvement in therapy and (2) wider availability and use of MR imaging for detection of symptomatic and asymptomatic CNS metastasis. Tumors with a high propensity to metastasize to the brain are lung cancer, breast cancer, renal cell carcinoma, and melanoma. About 14% of men and 8% of women with CNS metastatic tumor show no clear primary tumor and thus are diagnosed as carcinoma of unknown primary.
Molecular and genetic profile: CNS metastatic tumors mirror the molecular and genetic profiles of the original primary tumor of the body. Some molecularly defined tumor subtypes are more likely to metastasize to the CNS, such as erythroblastic leukemia viral oncogene homolog 2 (ERBB2)-positive and triple-negative breast cancer.
Clinical features and standard therapy: Surgical resection is reserved for large metastasis causing significant edema and mass effect. Gamma knife radiosurgery is used for multiple CNS metastases <2.5 cm in size. Whole brain radiation therapy is used for innumerable CNS metastases or leptomeningeal/dural metastases. Brachytherapy is used for recurrent CNS metastases. Targeted chemotherapy is used for CNS metastases from systemic cancer with specific molecular genetic alterations.
Imaging
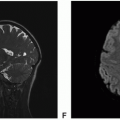
 Figure 18.1. Imaging of intraparenchymal cervical cancer metastasis with minimal edema. A. Axial fluid-attenuated inversion recovery (FLAIR): Large heterogeneously hyperintense intraparenchymal mass in the left occipital lobe with minimal surrounding vasogenic edema. B. Axial susceptibility-weighted imaging (SWI): Scattered blood products within the mass. C. Axial T1-precontrast: Mixed hypointense and isointense mass. D. Axial diffusion-weighted imaging (DWI): Mostly increased diffusion within the mass with rim of reduced diffusion. |
 Figure 18.1. (continued) E. Axial T1-postcontrast: Minimal to mild rim enhancement. F. Sagittal T1-postcontrast: Minimal to mild rim enhancement. |
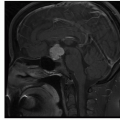
 Figure 18.2. Imaging of intraparenchymal endometrial cancer metastasis with moderate edema. A. Axial FLAIR: Large heterogeneously hypointense intraparenchymal mass in the left occipital lobe with moderate surrounding vasogenic edema. B. Axial T2: Markedly hypointense mass. |
 Figure 18.2. (continued) C. Axial T1-precontrast: Mixed hypointense and isointense mass. D. Axial DWI: Mostly increased diffusion within the mass with rim of reduced diffusion. E. Axial apparent diffusion coefficient (ADC): Mostly increased diffusion within the mass with rim of reduced diffusion. F. Axial SWI: Scattered blood products within the mass. G. Axial arterial spin labeling (ASL): Scattered areas of hyperperfusion within the rim of the mass (white arrows). H. Sagittal FLAIR: Heterogeneously hypointense mass with moderate surrounding vasogenic edema. |
 Figure 18.2. (continued) I. Axial T1-postcontrast overlayed with visual pathway tractography: Left occipital mass displaces the left lateral geniculate ganglion (yellow arrow) anteriorly and optic radiation (white arrows) laterally. J. Coronal T1-postcontrast: Irregular and nodular rim enhancement with large area of central necrosis. K. Sagittal T1-postcontrast: Irregular and nodular rim enhancement with large area of central necrosis. L. Axial T1-postcontrast: Irregular and nodular rim enhancement with large area of central necrosis and second enhancing nodule within the anterior lateral ventricle (yellow arrow). |
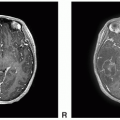
 Figure 18.3. Imaging of pancreatic mucinous adenocarcinoma metastases. A-F. Axial FLAIR: Multiple foci of parenchymal and leptomeningeal hyperintense lesions diffusely involving supra- and infra-tentorial brain. |
 Figure 18.3. (continued) G-L. Axial DWI: Reduced diffusion corresponding to the multiple foci of parenchymal and leptomeningeal hyperintense FLAIR lesions diffusely involving supra- and infra-tentorial brain.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|