Recent advances in understanding lymphatic disorders have significantly improved noninvasive imaging of the lymphatic circulation, especially in pediatric patients. The ability to obtain high-quality MR imaging using 3-dimensional reconstruction has transformed the display of the lymph vessels and substantially enhanced the ability to diagnose various pediatric lymphatic disorders. Real-time dynamic imaging adds functional information to the assessment. MR imaging is increasingly used, not only to assess but also as a follow-up after lymphatic disorder treatment. This article discusses up-to-date imaging techniques and clinical applications of dynamic magnetic resonance lymphangiography for assessing central conducting lymphatic anomalies.
Key points
- •
Magnetic resonance lymphangiography (MRL) in pediatric patients involves several aspects, such as clinical and laboratory workup, patient preparation, technique, and image optimization.
- •
Complimentary imaging with T2-weighted sequences is routinely performed in addition to dynamic MRL for evaluation of lymphatic disorders.
- •
Postprocessing of dynamic contrast-enhanced MRL images includes pregadolinium and postgadolinium subtraction, multiplanar reconstruction, and maximum intensity projection images, which help in improved evaluation of the lymphatic system.
- •
The central lymphatics are closely related to the intestinal, mesenteric, pleural, and pulmonary lymphatics, resulting in vice versa causality of abnormalities.
- •
Central conducting lymphatic anomaly is a commonly recognized abnormality on MRL from a variety of different causes.
Introduction
Current advances in understanding the pathophysiology of lymphatic disorders have raised immense interest in high-resolution imaging of the lymphatic system. A novel technique to directly access lymph nodes and inject radiographic contrast, when combined with improved MR imaging acquisition times, increased anatomic coverage, and superb postcontrast MultiPlanar Reconstruction (MPR), has revolutionized the imaging evaluation of the lymphatics in pediatric patients. The taxonomy, imaging interpretation, and treatment of lymphatic diseases based on dynamic magnetic resonance lymphangiography (MRL) are still evolving. This article reviews up-to-date imaging techniques and clinical applications of MRL for assessing lymphatic vessels and their abnormalities in the pediatric population.
Magnetic resonance lymphangiography technique
MR Imaging Optimization
Due to the small size and slow flow in lymphatic vessels, image optimization plays a crucial role in obtaining diagnostic quality high-resolution 3-dimensional (3D) volumetric images. Pediatric patients pose several unique challenges for MR imaging, such as inability to remain still and to follow breathing instructions. Such problems can be minimized by appropriate use of general anesthesia, sedation, and instructed breathing techniques tailored to each individual pediatric patient as detailed in the following sections.
Patient Preparation
Consent
The consent for the MRL, typically obtained from the parent or a legal guardian, should explicitly discuss the indication of the procedure, brief steps of the procedure, answers to clinical queries that the study will possibly help address, and risks of the procedure. Additionally, the benefits and limitations of alternative options, such as the conventional fluoroscopic lymphangiography and lymphoscintigraphy, should be discussed.
Indications for magnetic resonance lymphangiography
Most common indications for evaluating the lymphatic system include clinical manifestations related either to abnormal lymphatic flow or to abnormal lymphatic leak. MRL can be used for planning and as a follow-up imaging tool for medical, interventional, or surgical treatments in lymphatic diseases. These can be visualized with conventional fluoroscopic lymphangiogram; however, MRL provides the added advantage of obtaining high-quality cross-sectional anatomic information and real-time dynamic imaging. Conventional fluoroscopic lymphangiography is typically performed using lipiodol as a contrast agent, which has increased risk in comparison with gadolinium-based contrast agents in patients with right to left cardiac shunts and severe pulmonary insufficiency. Lymphoscintigraphy is a suitable option for peripheral lymphatic evaluation but it lacks spatial and temporal resolution, provides limited anatomic information, and exposes the patient to ionizing radiation. In addition, lymphoscintigraphy does not provide optimal evaluation of the central conducting lymphatics (CCLs).
Relevant clinical history
A detailed clinical history is an essential part of the evaluation process. The chronologic timing of events; presence of additional related symptoms; family history, past medical and surgical history, especially cardiac history; any evidence of intracardiac shunts; hepatic disease; pulmonary disease; and protein-losing enteropathy should be inquired about. This helps in optimizing the MRL procedure protocol.
Preprocedure laboratory testing
Certain laboratory testing can be helpful as a part of an evaluation of the lymphatic disorders and an attempt should be made to have these available before the MRL. These laboratory tests include but are not limited to complete blood count, hemoglobin, absolute lymphocyte count, electrolytes (sodium, potassium, calcium), blood glucose, blood urea nitrogen, total protein and albumin, serum triglycerides and cholesterol, liver function tests, serum levels of fat soluble vitamins, coagulation factors, immunoglobin levels (IgG, IgM), thyroid-stimulating hormone and free thyroxine, and fecal alpha-1-antitrypsin levels. In addition, renal functions are also assessed as a safety precaution before any gadolinium administration.
General anesthesia
All infants and young children (<10 years old) are placed under general anesthesia with endotracheal intubation for the procedure. Light sedation medication, such as lorazepam, can be used in slightly older children to reduce anxiety. Most children older than 15 years of age are able to tolerate MRL with local anesthetic at the site of groin access. Pediatric patients are first transferred to the MR imaging table in the preparation room and made to lie supine over the posterior element of the torso receiver radiofrequency coil. Based on child’s age, they are then placed under general anesthesia before accessing the lymph nodes in the groin. In infants and young children (≤5 years old), a controlled ventilation technique (ie, breath-hold) is required and it is important to discuss this with the anesthesiologist to obtain motion artifact–free imaging.
Drainage of fluid
Most pediatric patients with central lymphatic conduction abnormalities have ascites or pleural effusion. A large volume of fluid may cause dielectric artifacts during MR imaging, impairing image resolution. Thoracentesis or paracentesis of this fluid before MRL should considered, which could easily be performed in the preparation room using ultrasound guidance.
Accessing lymph nodes
Using ultrasound, inguinal lymph nodes are first identified bilaterally. In small children and patients with severe lymphatic flow anomalies, visualization of the lymph nodes can be challenging. A careful search with ultrasound, even extending far above the groin crease, should be performed to look for accessible lymph nodes. It is best to avoid lymph nodes overlying the femoral vessels to prevent inadvertent vessel entry. Additionally, the ability to securely reach the nodes or the connecting lines from outside the MR imaging gantry should be carefully considered when choosing access nodes and placement of connecting tubes.
An initial ultrasound is performed to select suitably sized lymph nodes in the inguinal areas. This can sometimes be challenging in pediatric patients with lymphatic reflux with dilated lymphatic channels in the groin who may not exhibit definitive lymph nodes. After sterilely preparing both inguinal regions, 22-gauge to 25-gauge hypodermic needles or 20-gauge to 22-gauge angiocatheters connected to long low-volume connecting tubes are used to access the lymph nodes. The placement of long connecting tubes allows the contrast to be injected from outside the bore of the magnet without moving the patient. It is important to prevent repeated traumatization to the lymph node capsule to avoid extravasation of contrast. The needle tip is positioned in the medulla and a few drops of sterile water or saline mixed with local anesthetic is gently injected to confirm optimal access without evidence of any extravasation. The tubing is then secured to the patient’s thigh and connected via a 3-way stopcock connected to 3 mL of contrast and 10 mL of saline or sterile water syringes.
Availability of a hybrid MR imaging and fluoroscopy unit allows initial confirmation of intranodal needle position with injection of iodinated contrast under fluoroscopy, followed by transfer of patient to the MR imaging suite. It is critical to minimize patient movement during transfer to and positioning in the MR imaging suite to prevent inadvertent needle dislodgement.
MR Imaging Technique
Currently intranodal MRL is only performed under 1.5-T magnets, although there are efforts to use the higher resolution properties of a 3-T scanner. Angiocatheters can be safely used for accessing the lymph nodes when imaging in a 3-T field. The coverage area includes upper third of the thigh to neck craniocaudally. A torso coil is typically used, which is adequate in small children but not in taller or older patients. In such taller or older pediatric patients, centering of the coil should be done at the region of interest based on clinical suspicion and questions that the MRL is being performed to address. The anterior receiver coil should be supported away from the sterile field with props or sheets to prevent needle displacement and field contamination. Adequate right to left coverage to image the central channels during volumetric imaging should be planned. Time to scan and breath-hold concurrently increases with larger coverage volume. These tradeoffs should be diligently well thought out and imaging should be planned accordingly.
MR imaging acquisition
The commonly performed MR imaging sequences during MRL include (1) T2-weighted imaging; (2) precontrast and postcontrast T1-weighted dynamic MR imaging; and (3) a precontrast and postcontrast steady-state free precession (SSFP), balanced, electrocardiogram-triggered sequence with fat-suppression, which provides good visualization of the vessels relationship to the lymphatic channels.
An initial survey and calibration is performed at each respective station. Before any contrast injection, a 3D SSFP sequence with fat-suppression is acquired in sagittal plane. The T2-weighted imaging is then obtained in the axial or coronal plane to evaluate the overall anatomy and any suspected abnormalities or vascular anomalies. A respiratory-triggered, heavily T2-weighted sequence can be performed to delineate the lymphatic channels. Following this, a precontrast coronal 3D spoiled gradient-recalled echo T1-weighted imaging with fat-suppression is acquired. These images are then evaluated at the work station and repeated if necessary for optimization. It is crucial to obtain good coverage and resolution of the T1-weighted precontrast images to be used as masks for subtraction after subsequent postcontrast imaging. The interventionalist then injects the contrast from outside the bore, without moving the patient, through the preplaced inguinal lymph node accesses via the long tubing.
For dynamic contrast-enhanced MR imaging, gadobutrol (macrocyclic nonionic gadolinium) at 0.1 mmol/kg of body weight is currently used. The calculated volume can be further diluted with normal saline to increase the final volume. Larger volumes of contrast solution are occasionally needed in pediatric patients with dysfunctional lymphatic channels, which act as high-capacitance vessels and are often associated with lymphatic reflux. A saline syringe is attached via a 3-way connector with the contrast-filled syringe and is used for chasing the gadolinium. Gadolinium is gently injected manually at a slow and well-controlled rate (0.5–1.0 mL/min). If there is any resistance experienced, the injection should be immediately stopped and the groin examined for any extravasation or tissue infiltration due to needle dislodgement.
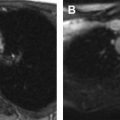
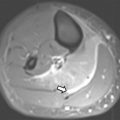
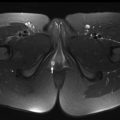
Postcontrast 3D spoiled gradient-recalled echo T1-weighted imaging with fat-suppression is intermittently repeated at approximately 30 to 45 seconds or longer, based on the transit rate of the contrast. An auxiliary monitor located in the MR imaging room can allow the physician operator to visualize the appearance of contrast and determine the time between sequential dynamic imaging without stopping the injection. Contrast first opacifies the iliac and lumbar lymphatic channels ascending cranially along the central lymphatics, cisterna chyli, and thoracic duct ( Fig. 1 A), which crosses the midline at the midthoracic level ( Fig. 1 B) to reach the neck, where it makes a posterior to anterior turn to terminate at the venous angle at the junction of the subclavian and internal jugular veins ( Fig. 1 C). Normally, gadolinium appears in the iliac and lumbar lymphatics within 1 to 2 minutes of injection; into the midline trunk by 2 to 3 minutes; within the cisterna chyli in 3 to 6 minutes; and, typically, in less than 10 minutes, it opacifies the thoracic duct and the terminal segment at the venous angle. When optimal visualization of the central lymphatic channels (cisterna chyli and thoracic duct) is noted, a 3D-SSFP postcontrast sequence can be acquired.

All contrast is washed out of the lymphatic channels in 15 to 20 minutes with the appearance of enhancement of renal parenchyma. Delayed imaging can be performed if needed. All the image data set is reviewed before concluding the study. The access needles are removed and appropriately disposed. The skin is observed for any local swelling or irritation. The parameters used for these sequences are detailed in Table 1 .
| Sequence | TR (ms) | TE (ms) | TI (ms) | FA (degrees) | Matrix (mm) | ST (mm) | NEX | Bandwidth (Hz) | Plane |
|---|---|---|---|---|---|---|---|---|---|
| 3D SSFP | 4.0 | 1.9 | 90 | 90 | 160 × 320 | 1.2 | 0.5 | 434 | Sagittal |
| Spoiled-GRE | 4.0 | 1.9 | 16 | 25 | 190 × 280 | 1.8 | 1 | 244 | Coronal |
| SSFSE T2-weighted | 4500 | 97 | 0 | — | 384 × 256 | 4 | 0.5 | — | Axial or coronal |
Postprocessing technique
The MR images can be initially assessed on the picture archiving and communication system (PACS) workstation for completion. Postprocessing is typically preformed on a dedicated postprocessing 3D workstation. MPR and postcontrast subtraction images are obtained from a 3D volumetric image data set. Two-dimensional MPR images are single-voxel thick images, which can be created and displayed along any selected planes, such as coronal, sagittal, or oblique planes. These images are very helpful to delineate, and resolve small caliber lymphatics and detect the site of abnormality. Maximum intensity projection (MIP) volume rendering images are reconstructed by selecting the highest signal voxels to improve visibility of the lymphatic channels and are normally reformatted in coronal plane. Interactive off-axis MIP images are especially helpful in delineating the course of the thoracic duct.
Magnetic resonance lymphangiography technique
MR Imaging Optimization
Due to the small size and slow flow in lymphatic vessels, image optimization plays a crucial role in obtaining diagnostic quality high-resolution 3-dimensional (3D) volumetric images. Pediatric patients pose several unique challenges for MR imaging, such as inability to remain still and to follow breathing instructions. Such problems can be minimized by appropriate use of general anesthesia, sedation, and instructed breathing techniques tailored to each individual pediatric patient as detailed in the following sections.
Patient Preparation
Consent
The consent for the MRL, typically obtained from the parent or a legal guardian, should explicitly discuss the indication of the procedure, brief steps of the procedure, answers to clinical queries that the study will possibly help address, and risks of the procedure. Additionally, the benefits and limitations of alternative options, such as the conventional fluoroscopic lymphangiography and lymphoscintigraphy, should be discussed.
Indications for magnetic resonance lymphangiography
Most common indications for evaluating the lymphatic system include clinical manifestations related either to abnormal lymphatic flow or to abnormal lymphatic leak. MRL can be used for planning and as a follow-up imaging tool for medical, interventional, or surgical treatments in lymphatic diseases. These can be visualized with conventional fluoroscopic lymphangiogram; however, MRL provides the added advantage of obtaining high-quality cross-sectional anatomic information and real-time dynamic imaging. Conventional fluoroscopic lymphangiography is typically performed using lipiodol as a contrast agent, which has increased risk in comparison with gadolinium-based contrast agents in patients with right to left cardiac shunts and severe pulmonary insufficiency. Lymphoscintigraphy is a suitable option for peripheral lymphatic evaluation but it lacks spatial and temporal resolution, provides limited anatomic information, and exposes the patient to ionizing radiation. In addition, lymphoscintigraphy does not provide optimal evaluation of the central conducting lymphatics (CCLs).
Relevant clinical history
A detailed clinical history is an essential part of the evaluation process. The chronologic timing of events; presence of additional related symptoms; family history, past medical and surgical history, especially cardiac history; any evidence of intracardiac shunts; hepatic disease; pulmonary disease; and protein-losing enteropathy should be inquired about. This helps in optimizing the MRL procedure protocol.
Preprocedure laboratory testing
Certain laboratory testing can be helpful as a part of an evaluation of the lymphatic disorders and an attempt should be made to have these available before the MRL. These laboratory tests include but are not limited to complete blood count, hemoglobin, absolute lymphocyte count, electrolytes (sodium, potassium, calcium), blood glucose, blood urea nitrogen, total protein and albumin, serum triglycerides and cholesterol, liver function tests, serum levels of fat soluble vitamins, coagulation factors, immunoglobin levels (IgG, IgM), thyroid-stimulating hormone and free thyroxine, and fecal alpha-1-antitrypsin levels. In addition, renal functions are also assessed as a safety precaution before any gadolinium administration.
General anesthesia
All infants and young children (<10 years old) are placed under general anesthesia with endotracheal intubation for the procedure. Light sedation medication, such as lorazepam, can be used in slightly older children to reduce anxiety. Most children older than 15 years of age are able to tolerate MRL with local anesthetic at the site of groin access. Pediatric patients are first transferred to the MR imaging table in the preparation room and made to lie supine over the posterior element of the torso receiver radiofrequency coil. Based on child’s age, they are then placed under general anesthesia before accessing the lymph nodes in the groin. In infants and young children (≤5 years old), a controlled ventilation technique (ie, breath-hold) is required and it is important to discuss this with the anesthesiologist to obtain motion artifact–free imaging.
Drainage of fluid
Most pediatric patients with central lymphatic conduction abnormalities have ascites or pleural effusion. A large volume of fluid may cause dielectric artifacts during MR imaging, impairing image resolution. Thoracentesis or paracentesis of this fluid before MRL should considered, which could easily be performed in the preparation room using ultrasound guidance.
Accessing lymph nodes
Using ultrasound, inguinal lymph nodes are first identified bilaterally. In small children and patients with severe lymphatic flow anomalies, visualization of the lymph nodes can be challenging. A careful search with ultrasound, even extending far above the groin crease, should be performed to look for accessible lymph nodes. It is best to avoid lymph nodes overlying the femoral vessels to prevent inadvertent vessel entry. Additionally, the ability to securely reach the nodes or the connecting lines from outside the MR imaging gantry should be carefully considered when choosing access nodes and placement of connecting tubes.
An initial ultrasound is performed to select suitably sized lymph nodes in the inguinal areas. This can sometimes be challenging in pediatric patients with lymphatic reflux with dilated lymphatic channels in the groin who may not exhibit definitive lymph nodes. After sterilely preparing both inguinal regions, 22-gauge to 25-gauge hypodermic needles or 20-gauge to 22-gauge angiocatheters connected to long low-volume connecting tubes are used to access the lymph nodes. The placement of long connecting tubes allows the contrast to be injected from outside the bore of the magnet without moving the patient. It is important to prevent repeated traumatization to the lymph node capsule to avoid extravasation of contrast. The needle tip is positioned in the medulla and a few drops of sterile water or saline mixed with local anesthetic is gently injected to confirm optimal access without evidence of any extravasation. The tubing is then secured to the patient’s thigh and connected via a 3-way stopcock connected to 3 mL of contrast and 10 mL of saline or sterile water syringes.
Availability of a hybrid MR imaging and fluoroscopy unit allows initial confirmation of intranodal needle position with injection of iodinated contrast under fluoroscopy, followed by transfer of patient to the MR imaging suite. It is critical to minimize patient movement during transfer to and positioning in the MR imaging suite to prevent inadvertent needle dislodgement.
MR Imaging Technique
Currently intranodal MRL is only performed under 1.5-T magnets, although there are efforts to use the higher resolution properties of a 3-T scanner. Angiocatheters can be safely used for accessing the lymph nodes when imaging in a 3-T field. The coverage area includes upper third of the thigh to neck craniocaudally. A torso coil is typically used, which is adequate in small children but not in taller or older patients. In such taller or older pediatric patients, centering of the coil should be done at the region of interest based on clinical suspicion and questions that the MRL is being performed to address. The anterior receiver coil should be supported away from the sterile field with props or sheets to prevent needle displacement and field contamination. Adequate right to left coverage to image the central channels during volumetric imaging should be planned. Time to scan and breath-hold concurrently increases with larger coverage volume. These tradeoffs should be diligently well thought out and imaging should be planned accordingly.
MR imaging acquisition
The commonly performed MR imaging sequences during MRL include (1) T2-weighted imaging; (2) precontrast and postcontrast T1-weighted dynamic MR imaging; and (3) a precontrast and postcontrast steady-state free precession (SSFP), balanced, electrocardiogram-triggered sequence with fat-suppression, which provides good visualization of the vessels relationship to the lymphatic channels.
An initial survey and calibration is performed at each respective station. Before any contrast injection, a 3D SSFP sequence with fat-suppression is acquired in sagittal plane. The T2-weighted imaging is then obtained in the axial or coronal plane to evaluate the overall anatomy and any suspected abnormalities or vascular anomalies. A respiratory-triggered, heavily T2-weighted sequence can be performed to delineate the lymphatic channels. Following this, a precontrast coronal 3D spoiled gradient-recalled echo T1-weighted imaging with fat-suppression is acquired. These images are then evaluated at the work station and repeated if necessary for optimization. It is crucial to obtain good coverage and resolution of the T1-weighted precontrast images to be used as masks for subtraction after subsequent postcontrast imaging. The interventionalist then injects the contrast from outside the bore, without moving the patient, through the preplaced inguinal lymph node accesses via the long tubing.
For dynamic contrast-enhanced MR imaging, gadobutrol (macrocyclic nonionic gadolinium) at 0.1 mmol/kg of body weight is currently used. The calculated volume can be further diluted with normal saline to increase the final volume. Larger volumes of contrast solution are occasionally needed in pediatric patients with dysfunctional lymphatic channels, which act as high-capacitance vessels and are often associated with lymphatic reflux. A saline syringe is attached via a 3-way connector with the contrast-filled syringe and is used for chasing the gadolinium. Gadolinium is gently injected manually at a slow and well-controlled rate (0.5–1.0 mL/min). If there is any resistance experienced, the injection should be immediately stopped and the groin examined for any extravasation or tissue infiltration due to needle dislodgement.
Postcontrast 3D spoiled gradient-recalled echo T1-weighted imaging with fat-suppression is intermittently repeated at approximately 30 to 45 seconds or longer, based on the transit rate of the contrast. An auxiliary monitor located in the MR imaging room can allow the physician operator to visualize the appearance of contrast and determine the time between sequential dynamic imaging without stopping the injection. Contrast first opacifies the iliac and lumbar lymphatic channels ascending cranially along the central lymphatics, cisterna chyli, and thoracic duct ( Fig. 1 A), which crosses the midline at the midthoracic level ( Fig. 1 B) to reach the neck, where it makes a posterior to anterior turn to terminate at the venous angle at the junction of the subclavian and internal jugular veins ( Fig. 1 C). Normally, gadolinium appears in the iliac and lumbar lymphatics within 1 to 2 minutes of injection; into the midline trunk by 2 to 3 minutes; within the cisterna chyli in 3 to 6 minutes; and, typically, in less than 10 minutes, it opacifies the thoracic duct and the terminal segment at the venous angle. When optimal visualization of the central lymphatic channels (cisterna chyli and thoracic duct) is noted, a 3D-SSFP postcontrast sequence can be acquired.