Chapter 4 Myocardium
Myocardial imaging
Imaging the ventricular myocardium is of critical importance for identifying patients with changes in myocardial size and mass. Further evaluation is required to understand why a particular patient may have changes in (1) myocardial shape or size and (2) myocardial function. The available imaging techniques can be divided into two groups.
The majority of techniques image the myocardial tissue directly:
 echocardiography (transthoracic 2D)
echocardiography (transthoracic 2D)
 CMR
CMR
 CT.
CT.
Other modalities image the myocardial tissue indirectly:
 Nuclear cardiology
Nuclear cardiology
Contrast and other injected agents
Contrast or other injected agents are usually used to optimize assessment of the myocardium. These increase the visibility of the myocardium, the blood flow through the tissue, and the metabolism within the tissue.
Injected agents can have the following properties.
 They flow through the microvessels (microbubbles, ultrasound contrast—myocardial contrast echocardiography (MCE)).
They flow through the microvessels (microbubbles, ultrasound contrast—myocardial contrast echocardiography (MCE)).
 They flow through the epicardial vessels and microcirculation (iodinated contrast agents—cardiac CT).
They flow through the epicardial vessels and microcirculation (iodinated contrast agents—cardiac CT).
 They flow through the microvessels and leak into the myocardium (gadolinium contrast agents—CMR).
They flow through the microvessels and leak into the myocardium (gadolinium contrast agents—CMR).
 They bind to the myocardium (radioactive tracers—nuclear cardiology).
They bind to the myocardium (radioactive tracers—nuclear cardiology).
 They are used within myocardial metabolism (radioactive tracers—PET).
They are used within myocardial metabolism (radioactive tracers—PET).
Agents are chosen because their unique properties mean that they provide a signal that can easily be identified by the imaging modality. The resolution of the imaging in this situation depends on the size of the agent used or, if the agent attaches to a particular cellular target, the size of that target.
Molecular imaging
Agents may become available that combine an agent easily seen with a particular imaging modality with a receptor or antibody that binds to a specific molecular target within the myocardium. This could be used to measure change in, for example, aspects of inflammation or ischaemia.
Possible causes of increased myocardial size or thickness include:
 hypertensive heart disease
hypertensive heart disease
 infiltrative cardiomyopathies
infiltrative cardiomyopathies
 hypertrophic cardiomyopathies
hypertrophic cardiomyopathies
 cardiac tumours.
cardiac tumours.
All these diseases can also lead to changes in function, typically evidence of diastolic dysfunction or a restrictive cardiomyopathy.
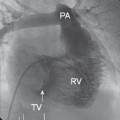
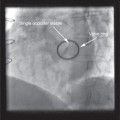
Masses in the heart
Cardiovascular imaging is essential in the identification and characterization of cardiac tumours. Echocardiography is usually the first modality to identify the mass and then further imaging with cardiovascular magnetic resonance of cardiac CT provides detailed assessment of position of mass, tissue characteristics and extent size.
Masses in the heart include:
Primary tumours (benign)
 myoxma
myoxma
 papillary fibroelastoma
papillary fibroelastoma
 lipoma
lipoma
 fibroma
fibroma
 rhabdomyoma.
rhabdomyoma.
Primary tumours (malignant)
 sarcomas
sarcomas
 angiosarcomas
angiosarcomas
 rhabdomyosarcomas
rhabdomyosarcomas
 primary lymphoma.
primary lymphoma.
Secondary tumours
 metastases.
metastases.
Cysts
Extra cardiac tumours
Echocardiography
Echocardiography is the most commonly used first-line investigational technique to assess the myocardium. Echocardiography provides assessment of:
 left ventricular size on standard 2D second-harmonic echocardiography
left ventricular size on standard 2D second-harmonic echocardiography
 myocardial function by Doppler imaging.
myocardial function by Doppler imaging.
Both may be observer dependent, and echocardiogrpahy has limited ability to dissect out differential diagnoses. Therefore more detailed imaging, typically with cardiovascular magnetic resonance, is usually warranted once echocardiography has identified myocardial disease.
Cardiac masses
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


