NASOLACRIMAL APPARATUS: BENIGN AND MALIGNANT TUMORS
KEY POINTS
- Imaging is required in almost all patients with benign and malignant tumors of the nasolacrimal apparatus.
- Imaging findings can markedly alter the medical decision making if a process other than tumor is identified.
- Imaging when tumors are known to be present can be used to identify the extent of disease and predict the likely morbidity of curative treatment.
Any orbital mass or disease process may be approached by first establishing whether it is preseptal (Chapters 70 and 71) or postseptal (Chapters 57–60, 62, and 64). Nasolacrimal apparatus problems are generally predominantly preseptal in their manifestations. The vast majority of these do not come to imaging, but almost all mass lesions will come to computed tomography (CT) and/or magnetic resonance imaging (MRI). This chapter considers nasolacrimal apparatus tumors and conditions that might mimic tumors.
The lacrimal sac and nasolacrimal duct are very unusual sites for origin of tumors. Most of the time, benign and malignant tumors of the skin (Chapter 71) or sinonasal region (Chapter 89) secondarily involve these structures. Carcinomas and rarely lymphoma may arise from the epithelium of the lacrimal drainage system.
Secondary acquired nasolacrimal duct obstruction (SALDO) is almost always due to an infectious or noninfectious inflammatory process (Chapter 68); however, this can also be caused by tumor intrinsic or extrinsic to the lacrimal drainage system (Fig. 69.1). Primary acquired nasolacrimal duct obstruction (PANDO) is a diagnosis that can be made only after tumor and other etiologies of the obstruction are excluded (Chapter 68).
ANATOMIC AND DEVELOPMENTAL CONSIDERATIONS
Applied Anatomy
The relevant anatomy of the nasolacrimal drainage system is discussed in detail in Chapter 44.
IMAGING APPROACH
Techniques and Relevant Aspects
The nasolacrimal drainage pathways are studied with CT and magnetic resonance (MR) techniques described in detail in Chapters 44 and 45. Specific CT protocols by indications are detailed in Appendix A. Specific MR protocols by indications are outlined in Appendix B. Almost all studies to investigate lacrimal drainage system obstruction potentially by tumor are done with contrast.
Pros and Cons
Masses of and around the lacrimal drainage system are studied primarily with CT with MRI held in reserve for selected cases.
CT typically is used to identify bone changes and survey the surrounding soft tissues for a likely infiltrating or obstructing mass. It is also used to determine whether the mass has extended to postseptal soft tissues or if there has been perineural spread involvement of regional lymph nodes.
MRI helps to characterize masses and to search for possible perineural spread better than CT. It is also used to determine whether the mass has extended to postseptal soft tissues; in this regard, it may be better than CT given that high-quality images are available. MR also helps to determine if perineural spread involvement of regional lymph nodes is present.
Dacryocystography may be useful to demonstrate an endoluminal mass, but it is generally nonspecific and does not add definitively to medical decision making.
Dacryoscintigraphy essentially is of no use.
Ultrasound is of no real clinical decision-making benefit.
Benign and Malignant Masses
Etiology
Primary tumors of the lacrimal drainage system are very rare (Fig. 69.1). The benign squamous cell papilloma is the most common of these rare lesions, and primary squamous cell carcinoma is the most common malignancy. Lymphoma may arise primarily in the lacrimal drainage system, although this also is unusual, being seen in <2% of biopsy specimens from nasolacrimal duct surgery (Fig. 69.2A,B). The lacrimal sac and duct are far more likely to be involved secondarily by skin and sinonasal malignancies than by cancers arising within the sac or duct (Fig. 69.2C–E). Eyelid tumors and skin cancers may involve the puncta and canaliculi.
Occasionally, tumors and other conditions within bone such as fibrous dysplasias will obstruct the lacrimal drainage system.
Prevalence and Epidemiology
Tumors arising in the nasolacrimal system are distinctly rare sporadic occurrences.


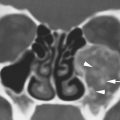
FIGURE 69.1. Two patients with masses presenting in the inferior and medial portion of the orbit. A–E: Patient 1. In (A), there is an abnormal mass in the lacrimal fossa region (black arrows) that seems to be contiguous with abnormal tissue in the nasal cavity (arrowheads). Compare to the normal nasolacrimal sac and duct region on the opposite side (white arrows). In (B), a section slightly posterior to that in (A) shows that the mass conforms to the anatomy of a distended nasolacrimal sac and duct (arrows). In (C), axial sections confirm that the mass is within the nasolacrimal drainage system (white arrow) and erodes bone (white arrowhead) compared to the normal side (black arrow). In (D), the T1-weighted (T1W) magnetic resonance imaging section on the same patient shows a mass extending along the nasolacrimal drainage system. The mass appears to likely be largely solid. In (E), the contrast-enhanced T1W image shows that the mass has a complex central portion (black arrowhead) and a thick, very enhancing wall (black arrow). Compare the normal nasolacrimal mucosa (white arrowhead) on the opposite side as well as the integrity of the lacrimal bone (white arrow) with that on the affected side. (NOTE: This was a primary adenocarcinoma arising along the nasolacrimal duct. However, from the imaging, it could also have been a distended and chronically inflamed system. There was inflammation as well as tumor present.) F, G: Patient 2. The patient formerly had a resection of an inverted papilloma and newly presented with a mass in the inferior medial aspect of the orbit. In (F), the solid mass affected the preseptal soft tissues and nasal cavity (white arrows). A mass could also be seen in the nasolacrimal canal (black arrow). In (G), the coronal reformation shows an inverted papilloma that invaded from its site of recurrence in the nasal cavity through the nasolacrimal drainage system into the preseptal soft tissues (arrows).
Related posts:
 Fibrous Dysplasia and other Fibro-osseous Lesions of the Craniofacial Skeleton
Fibrous Dysplasia and other Fibro-osseous Lesions of the Craniofacial Skeleton
 Intraconal Orbit: Tumors
Intraconal Orbit: Tumors
 Hypopharynx: Developmental Abnormalities
Hypopharynx: Developmental Abnormalities
 Tumors of the Submandibular Gland and Space and Tumorlike Conditions
Tumors of the Submandibular Gland and Space and Tumorlike Conditions
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


