NASOPHARYNX: DEVELOPMENTAL ABNORMALITIES
KEY POINTS
- The origin of a nasopharyngeal-level condition may not be well understood from the physical examination and may be considered threatening to one or more important and sometimes vital functions until its benign and possible congenital nature origin is established.
- Imaging typically will facilitate a precise diagnosis in these anomalies.
- Imaging will often significantly affect medical decision making in these developmental conditions.
- Computed tomography and magnetic resonance imaging are typically the main and frequently the only studies required.
- Imaging-guided biopsy may be useful in more difficult diagnostic cases when something other than a development mass is likely.
Developmental abnormalities usually present during childhood. Some manifest in infancy; however, the presentation may be delayed beyond infancy, sometimes well into the early adult years and even into middle age. Enlargement due to growth is variable. True growth may be at the same rate of normal structures, but masses may enter a rapid growth phase at times of accelerated growth of the individual—for instance, in adolescence. Some, such as high-flow vascular malformations, have internal physiologic dynamics that will allow them to enlarge more rapidly than normal tissues rather than truly proliferate. Others, such as branchial apparatus, dermoid, and epidermoid cysts, enlarge due to accumulation of contained secretions and sloughed cellular debris that has no exit. Enlargement may be due to infection, bleeding into the mass, and vascular thrombosis. Truly neoplastic developmental conditions such as teratomas or proliferative hemangioma (Chapters 8 and 9) will manifest growth out of proportion to normal structures.
Developmental abnormalities may be discovered incidentally on imaging studies done for other purposes. Some developmental conditions present as masses or because they interfere with function. In the nasopharynx, they tend to manifest with airway difficulties, often during infancy, since that age group is composed of obligate nasal breathers. These conditions are typically not painful unless there is some complicating factor present.
The natural history and imaging appearance of the more common developmental abnormalities that affect the nasopharynx are shown in the figures and chapters on those topics as follows:
- Branchial anomalies, duplication cysts, and related abnormalities and normal variants (Figs. 185.1–185.3 and Chapters 8 and 153)
- Disorders of pituitary migration (Figs. 185.4 and 185.5 and Chapter 79)
- Central meningoencephaloceles (Fig. 185.6 and Chapter 79)
- Epidermoid and dermoids cysts and teratomas (Fig. 185.7 and Chapter 8)
- Vascular malformations (Fig. 185.8 and Chapter 9)
ANATOMIC AND DEVELOPMENTAL CONSIDERATIONS
Embryology
The embryology of the conditions that affect the nasopharynx as presented includes that of the branchial apparatus presented in Chapter 153, migration of anterior pituitary anlage and related central skull base development described in summary form in Chapter 170, and vascular malformations discussed in Chapter 9.
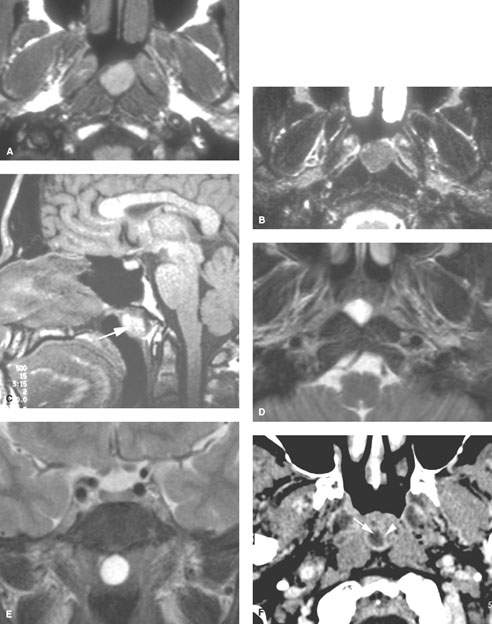
FIGURE 185.1. Four patients with Thornwaldt cysts. A, B: Patient 1. Magnetic resonance imaging of an incidental Thornwaldt cyst. In (A), the T1-weighted (T1W) image shows high signal intensity almost approaching that of fat. In (B), the T2-weighted (T2W) image shows the cyst contents to be much less intense than cerebrospinal fluid likely related to the mucoid nature of those cyst contents. C: T1W sagittal image in Patient 2 showing the typical position of a relatively high-density Thornwaldt cyst along the roof of the nasopharynx (arrow). D: Patient 3. T2W axial and coronal images to show the typical location of a Thornwaldt cyst, lying in the gutter between the prevertebral musculature, and in the coronal section in (E) showing no attachment to the skull base. F: Patient 4. Contrast-enhanced computed tomography study showing inflammation of the wall (arrowheads) surrounding an obvious fluid (arrow) collected within a Thornwaldt cyst.
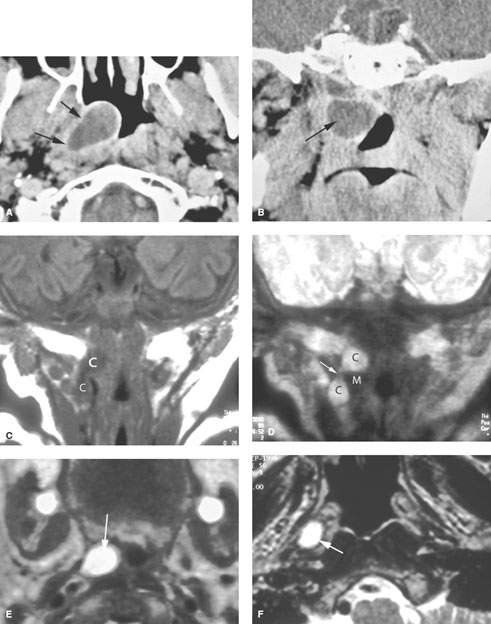
FIGURE 185.2. A, B: Patient 1 presenting with signs and symptoms of right eustachian tube obstruction shown on this study to be due to a cystic mass tracking along the eustachian tube (arrows) and subsequently shown to be epithelial line and presumed to be a first branchial pouch anomaly. C–E: Patient 2. Magnetic resonance imaging of an infant with a pharyngeal wall mass. The cystic structure (C) can be seen in both the T1-weighted (C) and T2-weighted (T2W) (D) images. Its appearance as it crosses the muscular (M) pharyngeal wall (arrow) to extend from the pharynx into the neck is an anatomic pattern unmistakably recognizable as a branchial apparatus anomaly. In (E), the T2W image shows the mass at the junction of the nasopharynx and oropharynx. F: Patient 3 had a long history of recurrent middle ear disease on the right. This submucosal cyst was obstructing the eustachian tube and was removed/marsupialized. It was found to be lined by respiratory epithelium and considered to be a duplication cyst.
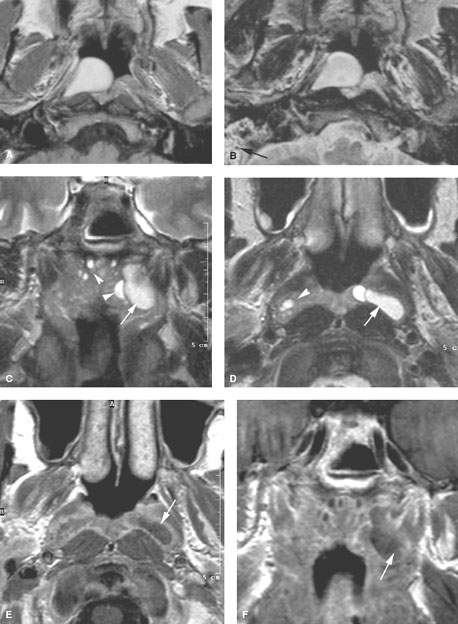

FIGURE 185.3. Two patients with inflammatory cysts within the nasopharynx that might mimic developmental cysts. A, B: Patient 1 presenting with right eustachian tube obstruction. The high-density material in the T1-weighted image in (A) suggests a mucoid content to the cyst. In (B), the heavily T2-weighted (T2W) images show that the contents are obviously fluid. Also note the fluid or mucosal thickening in the mastoid that was due to the eustachian tube obstruction (arrow). This was removed and found to be a large retention cyst within the fossa of Rosenmüller. C–G: Patient 2. T2W coronal (C) and axial (D) images showing what appears to be a large cyst within the fossa of Rosenmüller (arrow) with several smaller retention cysts present in the adenoidal tissue (arrowheads). The T2W axial image in (C) shows the larger cyst conforming to the fossa of Rosenmüller (arrow). In (E), enhancing mucosa can be seen surrounding the fluid content, suggesting that the cyst is within the lumen of the nasopharynx rather than deep to its muscular wall. In (F), the cyst is confirmed in the coronal plane to likely be mucosal and not penetrating or lying deep to the pharyngeal muscular wall. In (G), the T2W coronal image shows several retention cysts (arrowheads), including the front edge of the larger fossa of Rosenmüller cyst (arrow). (NOTE: Given the position and the associated retention cyst, this is more likely a retention cyst. This was proven to be true.)
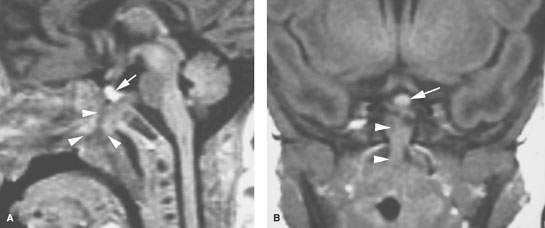
FIGURE 185.4. A patient presenting with noisy respiratory efforts. Magnetic resonance imaging was done because of a submucosal mass observed in the nasopharynx at endoscopy. A: T1-weighted (T1W) sagittal image showing a somewhat dysmorphic pituitary gland with no good differentiation between the anterior and posterior lobes (arrow). In addition, the craniopharyngeal canal is widened and leads to abnormal tissue within the nasopharynx occluding the airway above the soft palate (arrowheads). B: T1W coronal image showing the pituitary gland in a relatively normal position but dysmorphic abnormal tissue along the craniopharyngeal canal and projecting into the nasopharynx (arrowheads).
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Necrotizing (“Malignant”) Otitis Externa
Necrotizing (“Malignant”) Otitis Externa
 Hypopharynx: Developmental Abnormalities
Hypopharynx: Developmental Abnormalities
 Tumors of the Submandibular Gland and Space and Tumorlike Conditions
Tumors of the Submandibular Gland and Space and Tumorlike Conditions
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


