Nasopharynx: Noninfectious Inflammatory Conditions
KEY POINTS
- Imaging in noninfectious inflammatory diseases is generally nonspecific for the definitive diagnosis purposes but can lead to the next logical step in establishing a diagnosis.
- Atypical clinical and imaging features of nasopharyngeal pathology should raise the possibility of an inflammatory process.
- These diseases may be systemic, and indications of their systemic nature may be observed on computed tomography and magnetic resonance studies.
- These diseases and early nasopharyngeal cancers mimic one another, and both possibilities must be kept in mind when developing a plan of surveillance when the diagnosis is not established definitively.
After physical examination and in less definitive clinical situations, it may be difficult to decide whether an area of nasopharyngeal swelling is inflammatory as opposed to neoplastic. In a low-grade chronic inflammatory process, this distinction might remain unclear even after biopsy and watchful waiting might become the default strategy, sometimes with imaging surveillance as an aid. For instance, the nasopharynx may be the primary source of skull base osteomyelitis (Chapters 113 and 114) or secondarily involved by that disease. Imaging will be the prime determinant of the nature and extent of such a chronic infection and may be used as guidance for tissue sampling. This assistance in the diagnostic process might help to establish a definitive diagnosis such as one of the more unusual etiologies discussed in this chapter. Infectious inflammatory conditions are presented in Chapter 186.
ANATOMIC CONSIDERATIONS
Applied Anatomy
A thorough knowledge of nasopharyngeal anatomy and anatomic variations is required for the evaluation of inflammatory conditions of the nasopharynx. This anatomy is presented in detail with the introductory material on the nasopharynx (Chapter 184). These conditions may be contiguous with the skull base and temporal bone (Chapter 104); oropharynx (Chapter 190); and retropharyngeal, parapharyngeal, and masticator spaces (Section VI on the suprahyoid neck). Those chapters should be reviewed for both anatomic highlights and spread patterns of disease to develop a complete understanding of the regional spread patterns and related complications of these inflammatory conditions.
IMAGING APPROACH
Techniques and Relevant Aspects
Computed Tomography and Magnetic Resonance Imaging
Inflammatory conditions of the nasopharynx are studied with computed tomography (CT) and magnetic resonance imaging (MRI) in essentially the same manner as benign and malignant nasopharyngeal tumors, except the entire neck may not be included. The specifics and relative value of using these studies in this anatomic region are reviewed in Chapter 185. Problem-driven protocols for CT and MRI are presented in Appendixes A and B.
Other
Ultrasound has no definitive role in the evaluation of these inflammatory conditions. Radionuclide studies have modest contributions to make for chronic infectious disease (Chapter 5) and have little or no use in the entities in this chapter. They may be used in highly selected circumstances to monitor the response to therapy.
Pros and Cons
Inflammatory conditions in this region of the pharynx may involve or arise in the skull base and temporal bone, so CT may be done prior to magnetic resonance (MR) as a starting point depending on the initial dominant clinical findings (Fig. 187.1). However, MR will be more definitive in establishing the invasive nature of the process. MR should the primary imaging examination if there is an associated cranial neuropathy or any findings to suggest disease affecting the cavernous sinus. CT can be used for problem solving, such as in chronic conditions where it might help to establish the extent of temporal bone and skull base involvement.
SPECIFIC DISEASE/CONDITION
Systemic and Localized Noninfectious Inflammatory Diseases
Etiology
Wegener granulomatosis (WG) can manifest anywhere in the Waldeyer ring but does so most typically in the nasopharynx1,2 (Figs. 187.1–187.4). While sarcoidosis theoretically can manifest anywhere in the upper aerodigestive tract mucosa, the nasopharynx will usually be a site of contiguous disease in a patient with sinonasal involvement (Figs. 187.5 and 187.6). Langerhans cell histiocytosis only rarely involves the Waldeyer ring.
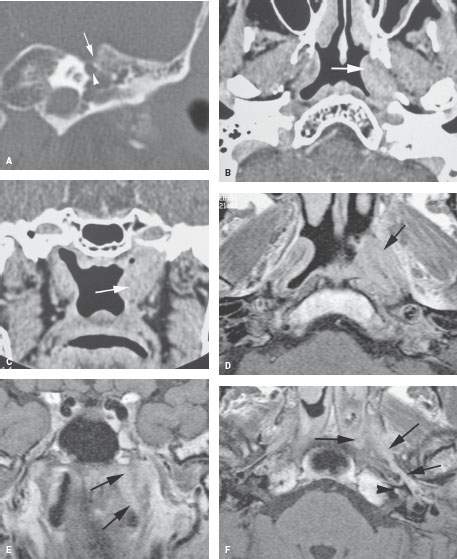
FIGURE 187.1. A patient presenting with left facial nerve weakness and signs and symptoms of eustachian tube obstruction and hearing loss. Computed tomography (CT) and magnetic resonance (MR) were done. A: CT study filmed for temporal bone detail showing erosion in the region of the first genu of the facial nerve (arrowhead) and the portion of the petrous apex just above (arrow). The mastoid and middle ear are filled with mucosal thickening, fluid, and/or some other tissue. B, C: Axial and coronal images from contrast-enhanced CT showing an infiltrating mass along the course of the eustachian tube up to its junction with the skull base (arrows). D–F: Contrast-enhanced T1-weighted images from the MR study. In (D), there is an infiltrating enhancing mass along the left eustachian tube (arrow). In (E), the enhancing mass can be seen infiltrating to the skull base (arrows). In (F), the abnormal enhancing tissue extends along the cartilage portion of the eustachian tube to its bony portion and then into the hypotympanum (arrows). There is also abnormal enhancement within the cochlea (arrowhead). (NOTE: Multiple biopsies of the nasopharynx returned inflammatory tissue. For that reason, circulating antineutrophil cytoplasmic antibody (c-ANCA) analysis was suggested, and that result was consistent with Wegener granulomatosis. The patient responded to cyclophosphamide.)
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Necrotizing (“Malignant”) Otitis Externa
Necrotizing (“Malignant”) Otitis Externa
 Hypopharynx: Developmental Abnormalities
Hypopharynx: Developmental Abnormalities
 Tumors of the Submandibular Gland and Space and Tumorlike Conditions
Tumors of the Submandibular Gland and Space and Tumorlike Conditions
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


