Zone 1
Clavicles and suprasternal notch to inferior aspect of cricoid cartilage
Zone 2
Cricoid cartilage to angle of mandible
Zone 3
Angle of mandible to skullbase
Patients with penetrating trauma to the neck who are hemodynamically unstable or display hard signs of vascular injury (expanding neck hematoma, arterial bleeding, bruit, pulse deficit) or aerodigestive tract injury (respiratory distress, crepitus, subcutaneous emphysema, hoarseness, hemoptysis, dysphagia) should undergo emergent neck exploration in the operating room. For stable patients, imaging is often invaluable for determining the extent of injury and further testing required, thus facilitating optimal patient management and guiding operative intervention.
Imaging Techniques
Computed tomography angiography (CTA) has become the modality of choice in the workup of hemodynamically stable patients with suspected vascular injury in the neck (i.e., carotid, jugular, vertebral vessels). As a result, the rate of surgical neck exploration, particularly negative exploration, has decreased over the past decade. Advantages of CTA include wide availability of multi-detector CT equipment capable of increasingly rapid scan times and reported sensitivity and specificity of 100 and 97 % respectively for the detection of clinically significant vascular and aero-digestive injuries to the neck. There is no difference in approach between penetrating and blunt trauma as long as the patient is stable.
Magnetic resonance imaging (MRI) and MR angiography (MRA) may also play a role. The advantages of MRI/MRA include improved detection of small infarctions and diffuse axonal injury compared to CT/CTA. Additionally, for patients suspected with cervical cord injury, MR assessment of the extra-cranial cerebral vasculature may be included among the sequences acquired during a single (although prolonged) imaging session. Studies evaluating the relative sensitivity and specificity of CTA versus MRI/MRA for the detection of carotid and/or vertebral artery dissection have been unable to show conclusive superiority of one modality over the other. The choice of imaging modality is typically based upon patient, availability, and equipment factors.
Vascular Trauma
Vascular injuries are among the most important of all potential injuries in the neck to recognize and treat expediently due to the high mortality with major arterial injury. Traditionally, Zone II injuries were often explored regardless of hemodynamic status in large part because of the relative ease of accessibility. Injury to Zones I and III required imaging confirmation of a vascular and/or aero-digestive tract injury due to poor exposure and difficulty in control of hemorrhage if the skull base or chest were involved. Mandatory operative exploration without clear injury in hemodynamically stable patients led to many negative explorations. Currently, selective operative management in hemodynamically stable patients has become standard. When evaluating neck injuries it is important to keep in mind that external wounds are not necessarily representative of the full extent of injury given that metallic and/or bone fragments may be deflected or otherwise travel along unknown trajectories through the soft tissues of the neck.
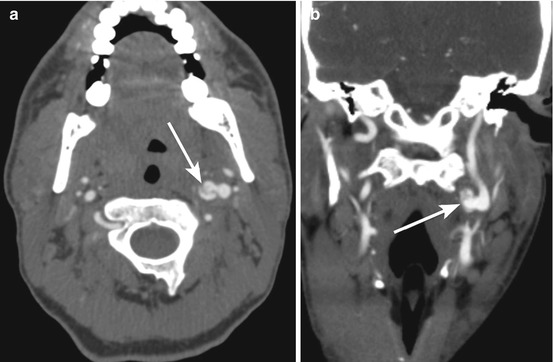
Both penetrating and blunt trauma may result in vascular injury in the neck (Figs. 42.1a, b and 42.2a, b). Even in the absence of penetrating trauma, blunt cerebrovascular injury may occur in over 1 % of patients sustaining significant blunt trauma and should be considered whenever patients exhibit neurological deficits without explanatory findings on brain imaging, major facial trauma or basilar skull fracture, cervical spine fractures, cervical bruit, high energy mechanism with neck flexion extension, near hanging, neck hematoma or “seat belt sign.” Evaluation for vascular injury in patients with neck trauma begins with CT angiography.
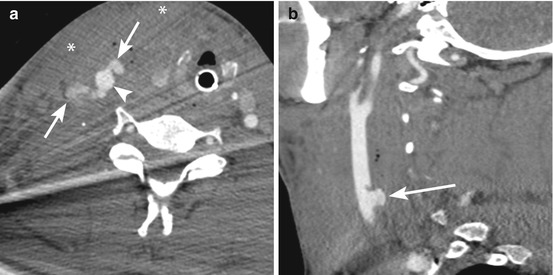
Fig. 42.1
Axial (a) and sagittal (b) images from a computed tomography angiogram (CTA) of a patient with a gunshot wound to the right neck. There is injury to the anterior and posterior aspects of the right common carotid artery (arrowhead) with active extravasation of contrast (arrows) consistent with active bleeding and associated large hematoma (asterisks). Note small amounts of streak artifact from bullet fragments