In the neonatal period the most frequently encountered spinal pathologies are of developmental nature. Spinal tumors or infections are exquisitely rare in neonates. Spinal trauma may occasionally be encountered and typically result from a complicated/traumatic delivery. This chapter will consequently focus on spinal malformations.
The development of the spinal canal and its contents is highly complex and involves multiple “programmed” anatomic and functional developmental and maturational processes. Malformations of the spinal canal and cord may be an isolated anomaly involving “only” the neuroaxis (brain and spinal cord/canal) or may be part of a complex syndrome or malformation (e.g., cloacal malformation). Next to the primary developmental etiology, the malformed spinal canal and cord may be secondarily injured because of prenatal, perinatal, or postnatal factors (e.g., long-standing exposure of the neural tissue to the amniotic fluid, mechanical injury during delivery, or postnatal infection). Detailed knowledge about normal neonatal spine imaging, as well as malformations, is essential to recognize malformations early (preferably prenatally) to counsel the parents during pregnancy, to plan possible intrauterine interventions, to make decisions about the mode of delivery, to optimize postnatal care, and to predict functional outcome.
In both the prenatal and postnatal period, ultrasound (US) and magnetic resonance imaging (MRI) give highly sensitive and specific information about the full extent and character of the spinal anomaly. Conventional radiography and computed tomography (CT) are rarely indicated and should be avoided to limit radiation exposure. In the following paragraphs the most common spinal malformations will be discussed based on their most apparent clinical findings.
Neonate With a Sacral Dimple
This is a common history seen in neonatal spinal sonography. Physical examination features that are more correlative with spinal abnormalities are dimple locations higher along the gluteal cleft or at lumbar level, larger or draining pits, and skin findings such as hairy patches and vascular anomalies. Sonography is an excellent initial evaluation for the spinal canal in the first few months of life because of the lack of ionizing radiation, relative ease of performing the examination, and presence of dorsal cartilage allowing sonographic window into the canal. Often, the sonographic findings are reassuring for normal spinal development. Features that are used to determine normal development are normal location of the conus medullaris at/above L2, normal appearance of a thin filum terminale, and normal pulsation of the cauda equina nerve roots. Pulsation of the conus can be documented with cine imaging or M-mode interrogation. The sonographic numbering of the vertebral bodies can be performed by counting caudal to cranial or by looking for the lumbosacral angle at L5-S1. Variants of normal that are frequently seen include a mildly prominent distal central canal (also known as ventricularis terminalis) and/or a filar cyst just below the conus.
Neonate With a Non-Skin-Covered Bump/Lesion at the Back
If there is no skin covering a spinal defect, the neural placode is exposed to the surface and is termed an open neural tube defect . If the neural placode is level with the adjacent skin, the lesion is classified as a myelocele (MC); if the neural placode is pushed outside of the hypoplastic/malformed osseous spinal canal, the neural placode appears raised in relation to the adjacent skin and will “pull out” the attached meninges, appearing as a bulging fluid-filled sac. Consequently, this lesion is classified as a myelomeningocele (MMC). Both lesions result from an incomplete or segmental defective closure of the neural tube in which the resultant neural placode did not detach from the adjacent surface ectoderm. The exposed surface of the neural placode should have become the inside of the neural tube, is consequently covered by ependyma, and leaks cerebrospinal fluid (CSF). The neural placode itself is believed to be less functional because of multiple complex primary and secondary processes, including the failure of closure itself with resulting deranged neuroarchitecture but also because of chronic injury as a result of the long-lasting exposure of the neural tissue to the amniotic fluid. Adjacent bone, muscle, and skin are also deficient in various degrees of severity. These malformations most frequently occur at the lumbosacral levels; however, the thoracic or cervical spinal cord may also be involved.
Furthermore, nearly all neonates with an open spinal dysraphism will have an associated Chiari type II malformation. It is believed that the chronic leakage of CSF at the level of the spinal dysraphia during the early second trimester is causative for the occurrence of an associated Chiari type II malformation. In several fetal centers around the world, based on this hypothesis, open spinal dysraphias are closed during intrauterine life with the goal to limit the severity of the Chiari type II malformation and to reduce the degree of associated hydrocephalus and possible need for ventriculoperitoneal shunt.
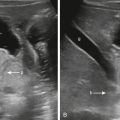
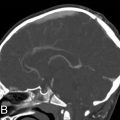
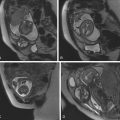
Identification of an open spinal dysraphism is often done on prenatal imaging (US and MRI) ( Figs. 29.1–29.3 ). A midline neural placode is seen either in level with the adjacent surface ectoderm (MC) or protruding like a bubble above the level of the surface ectoderm (MMC). Nerve roots appear along the anterior surface of the neural placode and, depending on the degree of neural placode protrusion, will appear “stretched” in their course toward the neural foramina. In MMC malformations, various degrees of meningeal structures will be encountered herniating lateral to the neural placode. The spinal canal is usually widened with absent or hypoplastic lateral and dorsal musculoskeletal structures. Infrequently, the neural placode may protrude asymmetrically outside of the malformed spinal canal. In addition, various degrees of hydromyelia may be encountered in the intact spinal cord superior to the spinal dysraphia. Within the cranial vault the typical stigmata of a Chiari type II malformation are encountered. Prenatal US typically identifies the spinal dysraphism and Chiari type II malformation, and fetal MRI is typically used to increase the level of anatomic detail and should focus on evaluating additional malformations or complications ( Fig. 29.4 ). Fetal MRI is especially helpful for the complete diagnostic workup of the Chiari II malformation (see Fig. 29.1 ). The associated findings often determine the long-term motor and neurocognitive outcome.




Neonate With a Skin-Covered Bump/Lesion at the Back
Skin-covered focal bumps/lumps along the midline of the neonatal back have a significantly better functional and neurocognitive prognosis than the non-skin-covered spinal dysraphias. In skin-covered dysraphias (closed neural tube defects) the neural placode is covered/protected by skin and subcutaneous tissue, limiting injury during intrauterine life. In addition, no leakage of CSF is observed; consequently, Chiari type II malformations are typically not seen. Depending on the degree of herniation of the neural placode outside of the malformed/hypoplastic osseous spinal canal and the size of the associated subcutaneous lipoma, these spinal dysraphias are categorized as myeloschisis with intradural lipoma, lipomyelocele (LMC), or lipomyelomeningoceles (LMMCs).
These skin-covered spinal dysraphias are believed to result from a premature dysjunction of the neural tube from the adjacent surface ectoderm before the neural tube has completely closed. The associated lipoma attached to the neural placode is believed to result from the interaction of adjacent mesodermal cells with the inner lining of the nonclosed neural tube during development, which induces the development of excessive amounts of fat. The resultant lipoma is consequently in close contact to the neural placode. Depending on the amount and extension of the fat, variant size lipomas occur that may be located exclusively intradural or may extend through the osseous defect into the subcutaneous region. On clinical inspection, significant lumps/bumps may be seen. Furthermore, cutaneous stigmata, including hairy tufts or focal skin discolorations, may be seen overlying the dysraphia. LMCs and LMMCs most frequently occur in the lumbar region.
Most children have a normal neurocognitive development but may require urological, orthopedic, and gastroenterological assistance. Their long-term morbidity consists mostly of neurogenic bladder dysfunction with possible renal damage if not treated appropriately.
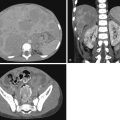
Prenatal and postnatal neuroimaging (US and MRI) rely on the identification of the osseous defect with a fat-covered neural placode within the level or dorsally of the osseous defect ( Figs. 29.5 and 29.6 ). Similar to the open spinal dysraphias, the closed malformations are classified depending on the amount of tissue that is protruding outside of the spinal canal. The spinal cord is often tethered. If no significant lipoma is present, the skin-covered spinal dysraphias may be easily missed by prenatal US. Fetal MR usually displays the skin-covered spinal dysraphia in better detail but may also occasionally fail to identify the anomaly. T1-weighted MR sequences may be helpful for identification of the T1-hyperintense lipoma. Chiari type II malformations are exquisitely rare in skin-covered spinal dysraphia. The size of the lipoma can vary significantly and may pose a large cosmetic issue for the child, especially as the child grows older. Surgical reduction of the lipoma is frequently performed later in life. A precise identification of the interface between the lipoma and the neural placode is essential for guiding surgical correction. A large lipoma may exert massive mass effect on the neural placode, even resulting in partial rotation of the neural placode with asymmetric protrusion of meninges outside of the level of the spinal canal. Finally, evaluation for additional associated malformations is important, for example, urogenital or anorectal malformations.


Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


