Fig. 14.1
Male patient. Carcinoma of the bulbous urethra. (a) Voiding cystourethrography shows an irregular stenosis (arrowheads) at the level of the bulbous urethra with marked dilatation of the posterior urethra (*). (b) Retrograde urethrography is more accurate for evaluating the proximal portion of the stenosis (arrowheads)

Fig. 14.2
Female patient. Carcinoma of the urethra. Voiding cystourethrography shows a severe irregular stenosis at the level of the middle urethra (arrowhead)
Ultrasound
High-resolution transperineal, transrectal, and transvaginal ultrasound are reliable for urethral abnormalities.
Retrograde sonourethrography allows an excellent evaluation of the anterior penile urethra. Normal saline solution is introduced to distend the lumen and create a good contrast with adjacent tissue. Intraluminal lubricant and anesthetic jelly can also be used. The posterior portion of the penile urethra can be investigated using linear high-frequency endorectal probes; transperineal sonography is less accurate.
Transvaginal and transrectal ultrasound provide the best evaluation of the female urethra.
Urethral carcinoma appears as a hypo- to isoechoic, irregularly marginated lesion. Ultrasound is able to identify the mass and the associated urethral stricture and can detect the spread into the surrounding periurethral tissue (Figs. 14.3 and 14.4).
Fig. 14.3
Male patient. Carcinoma of the bulbous urethra. (a) Longitudinal ultrasound scan. Voiding sonourethrography shows a tumor mass (M) with extensive infiltration of the corpus spongiosum (curved arrows) causing severe stenosis of the urethra. The urethral lumen is dilated proximal to the lesion (*) and not distended distal to the lesion (arrowheads). (b) Axial ultrasound scan. Retrograde sonourethrography shows the distal portion of the mass (M) infiltrating the corpus spongiosum. The urethral lumen (arrowheads) is irregular and stenotic. (c) Longitudinal ultrasound scan at the base of the penis showing the mass (M) infiltrating the corpus spongiosum (curved arrows) and the corpora cavernosa (CC)
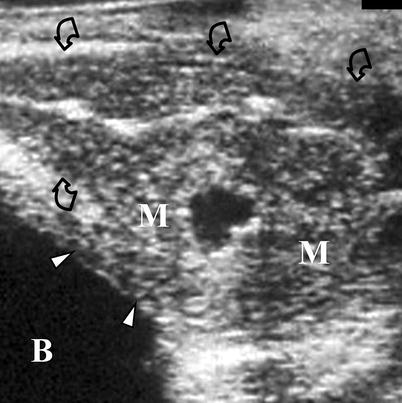
Fig. 14.4
Female patient. Urethral carcinoma. Longitudinal transrectal ultrasound scan demonstrates a urethral tumor mass (M) infiltrating the vagina (curved arrows) and the base (arrowheads) of the urinary bladder (B)
Computed Tomography
In some centers, CT is the most commonly used procedure for imaging the local extent and pelvic spread of urethral malignant disease. The accuracy of the technique, however, is limited both in female and in male by the low contrast resolution compared to MR imaging (Fig. 14.5).

Fig. 14.5
Male patient with urethral cancer. Contrast-enhanced coronal CT image showing a mass (*) replacing the bulbar portion of the corpus spongiosum. No cleavage is appreciable between the mass, corpora cavernosa (arrowheads), and the soft tissues of the scrotal root. The tunica albuginea of the corpora cavernosa is not interrupted
In female patients, in particular, the difficulty in differentiating the vagina from urethra and therefore detecting tumor involvement of the anterior vaginal wall is a major limitation of this modality. Moreover, evaluation of involvement of the base of the urinary bladder is problematic because tumor and bladder wall have similar CT attenuation.
Major indications of CT scan in patients with urethral malignancies are evaluation of nodal disease and identification of pulmonary, cerebral, hepatic, adrenal, and other abdominal metastases. Nodal enlargement, however, is nonspecific for malignancy, and distant metastases are uncommon at first examination and are reported to occur in only 10–15 % of advanced cancer (Fig. 14.6).
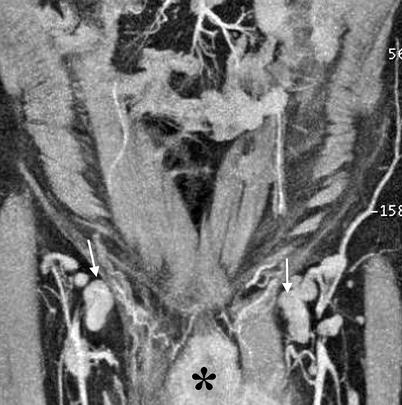
Fig. 14.6
Male patient with urethral cancer. MIP image of contrast-enhanced CT reveals the urethral mass (*) and bilaterally enlarged inguinal nodes (arrows)
Magnetic Resonance Imaging
The value of MR imaging in the detection and characterization of urethral tumors is limited. In fact, small lesions may be overlooked, and differential diagnosis between benign and malignant pathologies may be difficult. The appearance of benign granulation tissue and that of malignant tumors, in particular, may be similar. With its multiplanar capability and high tissue contrast, MR imaging is widely used for local staging of urethral cancer both in men and women. In men, it is especially useful for those tumors that invade the root of the penis for which a comprehensive physical examination is often limited.
In female patients, a study reports that MR imaging is 80 % accurate in showing tumor extension to the periurethral adipose tissue and 73 % accurate in showing invasion of the anterior vaginal wall (Fig. 14.7). MR imaging is effective also in evaluating infiltration of the bladder wall and pelvic vascular involvement (Fig. 14.8).
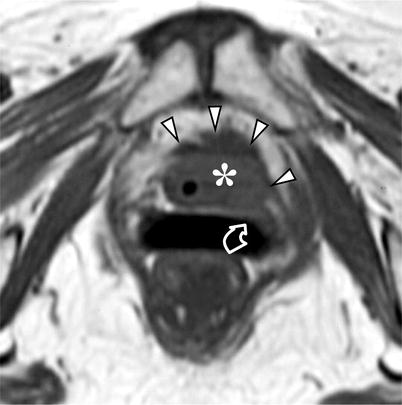
Fig. 14.7
Female patient with urethral cancer. Axial T1-weighted MR image demonstrates a urethral mass (*) with irregular margins infiltrating the periurethral adipose tissue (arrowheads) and the anterior wall of the vagina (curved arrow)

Fig. 14.8
Female patient with urethral cancer. Sagittal gadolinium-enhanced T1-weighted MR image demonstrates the urethral tumor (*) infiltrating the urinary bladder (curved arrow) and the anterior wall of the vagina (arrowheads)
The reported accuracy of MR imaging for pelvic and abdominal lymph node staging is similar to CT. Preliminary investigations using lymphotropic contrast agents show promising results in differentiating reactive from malignant nodes in pelvic cancers. No data, however, have been reported on urethral tumors.
At MR imaging, urethral cancer is seen in males as a soft tissue mass along the course of the urethra with similar or lower signal intensity on T1-weighted images and lower signal intensity on T2-weighted images compared to that of the surrounding corpus spongiosum. Sometimes high signal intensity on T2-weighted images is observed, due to associated inflammation.
After gadolinium administration, the tumor usually shows mild enhancement and therefore presents with lower signal intensity than the surrounding corpus (Fig. 14.9). Tumor extension into the penile bodies can be demonstrated on T2-weighted and contrast-enhanced T1-weighted images.
Fig. 14.9
Male patient. Carcinoma of the bulbous urethra. Sagittal T2-weighted (a) and gadolinium-enhanced T1-weighted (b) MR images show the mass (*) infiltrating the root of the corpora cavernosa (curved arrow)
Rarely, the urethral tumor can arise from the Cowper’s gland and may be seen as soft tissue mass in the urogenital diaphragm where the Cowper’s gland is located.
Only sporadic cases of other primary malignancies of the urethra evaluated with MR imaging have been reported in the literature.
Squamous cell carcinomas are hypointense on T2-weighted images and show heterogeneous contrast enhancement.
At MR imaging, transitional cell carcinomas appear as lobulated masses that are iso- to hypointense on both T1- and T2-weighted images and demonstrate heterogeneous contrast enhancement.
Adenocarcinoma appears as a heterogeneously enhancing, exophytic tumor commonly located in a diverticulum. At MR imaging, it shows high signal intensity on T2-weighted images with a low-intensity peripheral rim and variable contrast enhancement.
Nuclear Medicine
Skeletal scintigraphy is the most sensitive method for detecting bone metastases which in fact are very rare in patients with urethral cancer. PET/CT reduces the limitations of CT and MR imaging in detection of metastatic nodal involvement in other pelvic malignancies; no studies, however, evaluated patients with urethral cancer.
Pathology
Primary urethral carcinoma occurs more often in females than in males but is rare in both. Cancers that arise in the prostatic urethra in males and in the proximal third of the urethra in females are almost always typical urothelial carcinomas, similar to those that arise in the urinary bladder.
It should be noted that the great majority of urothelial cancers in these sites arise in association with urinary bladder urothelial carcinoma, synchronously or metachronously.
Cancers arising in the membranous, bulbous, or penile urethra in men and in the distal two-thirds of the urethra in women are more often of squamous cell type, rather than urothelial (Fig. 14.10). Primary urethral adenocarcinoma is exceptionally rare in males but does account for a small minority of female cases.

Fig. 14.10
Primary squamous cell carcinoma of male urethra. Patient was a 27-year-old male, without a prior history of malignancy or any known predisposing conditions prior to discovery of this lesion. The gray-white lesion (arrow) infiltrated periurethral soft tissues (From MacLennan GT, Resnick MI, Bostwick DG. Pathology for urologists. Philadelphia: Saunders; 2003, with permission)
Primary prostatic urethral tumors in men often present at a high stage and can be difficult to treat. Consequently, the 5-year survival rates for such tumors are in the range of 20 %. Primary distal urethral cancers in men are usually found at an earlier stage, and about two-thirds of patients survive 5 years (Figs. 14.11 and 14.12).

Fig. 14.11
Primary urothelial carcinoma of male urethra. A white irregular tumor involves the urethra and adjacent erectile tissue. Patient had no prior history of urothelial carcinoma involving sites proximal to this lesion (Image courtesy of Liang Cheng, M.D.)
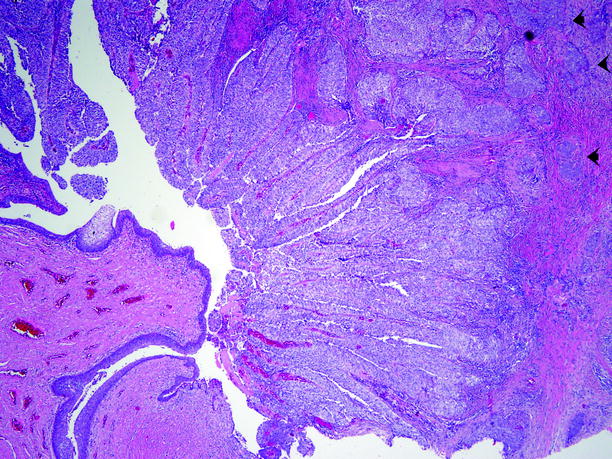
Fig. 14.12
Primary urothelial carcinoma of male urethra. Section from the lesion shown in Fig. 14.11. A papillary carcinoma partially fills the urethral lumen and infiltrates corpus spongiosum (arrows)
Primary malignant urethral tumors in women can mimic common benign urethral lesions clinically and are sometimes found unexpectedly in surgical specimens excised with a preoperative diagnosis of urethral diverticulum or urethral caruncle (Fig. 14.13).
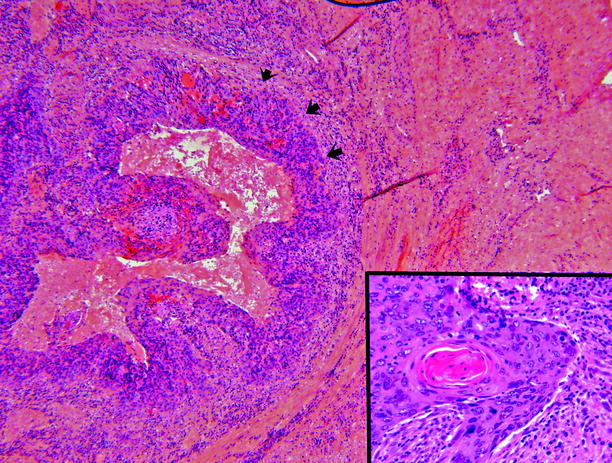
Fig. 14.13
Squamous cell carcinoma of female urethra. Patient underwent excision of a lesion that was clinically a suburethral diverticulum, but histologic evaluation showed an infiltrative neoplastic lesion (arrows). Invasive squamous cell carcinoma was found (inset)
Squamous cell carcinoma accounts for about three-quarters of primary urethral carcinomas in females; the remainder are urothelial carcinomas and adenocarcinomas.
The histologic findings in urothelial carcinomas, squamous cell carcinomas, and adenocarcinomas arising primarily in the urethra in men and women are entirely similar to those that occur in the urinary bladder and have been described in Chap. 11.
Urethral Metastases
Ultrasound
Urethral metastases present at ultrasound as nodules of variable echogenicity and vascularization. Metastatic involvement from adjacent organs can present with diffuse infiltration of the urethra and surrounding tissues (Fig. 14.14).
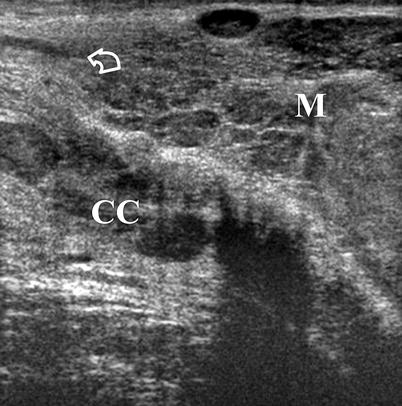
Fig. 14.14
Male patient with metastatic involvement of the urethra from bladder cancer. Longitudinal ultrasound scan demonstrates recurrent tumor (M) infiltrating the corpus spongiosum (curved arrow) and the corpora cavernosa (CC)
Magnetic Resonance Imaging
On T2-weighted images, urethral metastases show intermediate signal intensity. Invasions from other malignancies may be evaluated more appropriately on MRI.
Pathology
Involvement of the urethra by a distant cancer is uncommon. It may occur by direct contiguous extension of cancers of the bladder, prostate, penis, or gastrointestinal tract or by hematogenous spread from a more distant site (Figs. 14.15 and 14.16).

Fig. 14.15
Metastatic cancer involving urethra. Patient had invasive high-grade urothelial carcinoma of the bladder that metastasized to the penis, forming an expansile nodule that filled the corpora cavernosa and eroded the urethra (arrows)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree