Neuroblastoma
 Background
Background
What are the 3 types of neuroblastic tumors?
3 types of neuroblastic tumors:
1. Neuroblastoma (NB)
2. Ganglioneuroblastoma
3. Ganglioneuroma
These tumors differ in the degree of cellular maturation.
What are the 4 most common malignancies of childhood?
4 most common malignancies of childhood:
1. Leukemia
2. Brain tumors
3. Lymphoma
4. NB
What is the most common malignancy in infants?
NB is the most common malignancy in infants.
Estimate the annual incidence of NB in the U.S.
There are ∼650 cases/yr of NB in the U.S.
What is the median age at Dx for NB?
The median age at Dx is 17 mos, with a range between birth and 15 yrs. NBs in adults are rare and tend to have slower growth rate than in children.
Name 3 genetic syndromes associated with NB.
3 genetic syndromes associated with NB:
1. NF
2. Hirschsprung Dz
3. Fetal hydantoin syndrome
What tests have been used to screen infants for NB?
Historically, infants were screened for NB using urinary catecholamines (vanillylmandelic acid/homovanillic acid).
Does screening improve survival in NB?
This is controversial. Screening infants for NB with urinary catecholamines has been evaluated in multiple studies; however, the value of catecholamine-based screening is limited by its false+ rate and b/c a significant % of infant NBs spontaneously regress.
What markers distinguish NB from other small round blue tumors?
NB-specific markers:
1. Neuron-specific enolase
2. Synaptophysin
3. Neurofilament
What is the cell of origin for NB?
NB arises from neural crest cells of the sympathetic ganglion.
What % of NB pts have detectable urinary catecholamines?
90%
What genetic changes are associated with n-myc amplification?
Double-minute chromatin bodies and homogeneously staining regions are associated with n-myc amplification.
What are the genetic/chromatin changes that portend a poor prognosis in NB?
Genetic/chromatin changes with a poor prognosis in NB:
1. n-myc amplification
2. LOH 1p + 11q
3. diploid DNA
4. ↑ telomerase activity
In which pts does DNA content not have prognostic importance?
DNA content does not have prognostic importance in metastatic pts.
What % of NB pts present with n-myc amplification?
30%–40% of pts present with n-myc amplification. An n-myc amplification is associated with poor prognosis.
What % of NB pts present with 1p deletions?
70% of pts present with 1p deletions.
What is the genetic variation on 6p22 that is associated with clinically aggressive NB?
Homozygosity for 3 single nucleotide polymorphisms on 6p22 is associated with stage IV Dz, n-myc amplification, and Dz relapse. (Maris JM et al., NEJM 2008)
What are the most common sites of presentation for NB?
Adrenal medulla > paraspinal > postmediastinum
In what age group is thoracic presentation of NB more common?
Thoracic NB is more common in infants.
What are some presenting Sx of NB?
Along with the presentation of a mass, NB may be associated with constitutional Sx (fever, malaise, pain, weight loss), periorbital ecchymosis (“raccoon eyes”), “blueberry muffin” sign (nontender blue skin mets), scalp nodules, bone pain, irritable/ill appearance, diarrhea (↑ vasoactive intestinal peptide), Horner syndrome, opsomyoclonus truncal ataxia (rare paraneoplastic syndrome of ataxia, random eye movement, and myoclonic jerking associated with early stage but persists after cure), and Kerner-Morrison syndrome (diarrhea, low K).
What % of NB pts present with mets overall? How does this differ by age?
75% of all NB pts present with mets overall. 60% of pts <1 yr present with localized disease, while 70% of patients >1 yr present with mets.
What are the most common sites of mets for NB?
NB commonly metastasizes to bone (∼50%), LNs (35%), BM, liver, skin, and orbits. Lung mets are rare.
What are the most common bony sites of metastatic Dz in NB?
Bones of the skull and orbit (proptosis, ecchymosis, scalp mass)
What features distinguish NB from Wilms tumor?
(1) NB (85%) is more likely to exhibit calcifications vs. 5%–10%, in Wilms, (2) median age of presentation for NB is 1 yr vs. 3.5 yrs for Wilms, (3) Wilms is more common in African Americans, (4) Wilms patients appear healthy vs. NB patients appear sick, (5) Wilms arises from and destroys the kidney vs. NB displaces the kidney, (6) NB can cross midline (Wilms does not), (7) NB rarely metastasizes to the lungs (Wilms can metastasize to the lungs).
What are the classic histologic findings seen in NB?
Homer-Wright pseudorosettes, hemorrhage, and calcification
Does screening change the mortality rate of NB?
No. The Quebec project increased the detection rate of NBs but failed to have an impact on mortality in the screened populations. The high spontaneous regression rate led to overdiagnosis of clinically insignificant Dz.
 WORKUP/STAGING
WORKUP/STAGING
Outline the workup for pts with suspected NB.
Suspected NB workup:
1. H&P
2. Labs (CBC, BUN/Cr, LFTs, serum markers, UA, urine catechol)
3. Imaging of primary: CT C/A/P, abdominal US, or MRI abdomen/liver/spine)
4. Workup of mets (bone scan, I-131 metaiodobenzylguanidine [MIBG] scan, BM Bx, CT/MRI as needed)
5. Pathology (DNA content, n-myc amplification, and cytogenetics)
Why is a BM Bx important in the workup of NB?
BM Bx may obviate the need for primary site surgery if the testing is positive and the clinical picture is clear.
What % of NB pts have uptake on an I-131 MIBG scan?
∼90% of NB pts have uptake on an I-131 MIBG scan.
What are the currently used NB staging systems?
As of 2010, most cooperative group trials use the International Neuroblastoma Staging System (INSS), which involves the extent of surgical resection. However, a new staging system that uses only pre-Tx factors has been developed: the International Neuroblastoma Risk Group (INRG). These 2 staging systems will likely be used concurrently to allow for comparisons between trials. (Monclair T et al., JCO 2009)
Summarize the INSS staging system.
Stage 1: unilat localized tumor s/p GTR +/– microscopic residual Dz; ipsi LN–, though LNs attached and removed with the primary may be involved
Stage 2A: unilat localized tumor s/p STR only; ipsi LN–, though LNs attached and removed with the primary may be involved
Stage 2B: unilat localized tumor s/p GTR or STR with involved non-adherent ipsi LNs; enlarged contralat LN–.
Stage 3: unresectable localized tumor extending across the midline +/– regional LN involvement; unilat localized tumor with contralat regional LN involvement
Stage 4: distant Dz except as defined by stage 4S
Stage 4S: localized unilat primary as defined by stage 1, 2A, or 2B; distant Dz limited to the liver, skin, and/or <10% of BM in infants <1 yo
What are the prognostic factors in NB per INRG?
Age, stage, histologic category, grade, n-myc amplification, 11q aberration, DNA ploidy
Summarize the INRG staging system.
In the INRG system, locoregional tumors are staged L1 or L2 based on the absence or presence of 1 or more of 20 image-defined radiographic findings (IDRFs). These IDRFs generally affect whether or not a tumor is surgically resectable and to what degree. The authors of the INRG system avoided the terms resectable and unresectable since that may depend more on the surgeon’s style and subjective judgment. Metastatic tumors are defined as stage M, except for stage MS, in which mets are confined to the skin, liver, and/or BM in pts <18 mos old. (Monclair T et al., JCO 2009)
What is the INRG stage of an 8-mo-old pt with metastatic Dz to bone only?
An 8-mo-old pt with metastatic Dz to bone only is INRG stage M (only BM, liver, and skin mets qualify for stage MS).
What is the INSS stage of a 14-mo-old pt with metastatic Dz to BM only?
A 14-mo-old pt with metastatic Dz to bone marrow only is INSS stage 4 (only pts <12 mos old qualify for stage 4S).
What 2 clinical factors are most predictive of cure in NB?
The 2 clinical factors most predictive of cure are age and stage at Dx.
In children with metastatic Dz, what is the most important prognostic factor?
In children with metastatic Dz, age (<1 yo best) is the strongest prognostic factor, even more so than n-myc.
The Shimada classification system divides NB into what 2 categories? What 5 features are used to classify pts in this system?
The Shimada classification system divides NB into favorable histology (FH) and unfavorable histology (UH). Favorable factors:
Stroma-rich (Schwann cell stroma)
Age (young)
Differentiation (well differentiated)
Mitotic/karyorrhectic index (low)
Nodularity (nonnodular)
(Mnemonic: Dr. Shimada has a SAD MiNd)
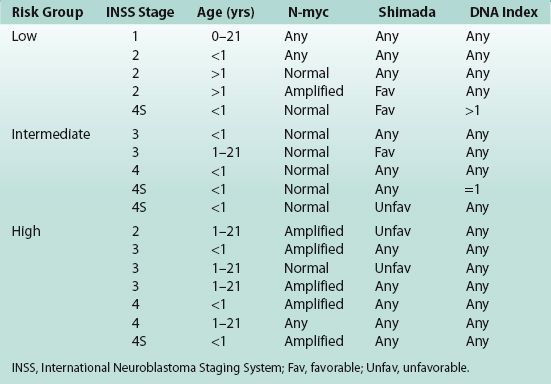
What 5 factors are used to classify NB pts into low-, intermediate-, and high-risk groups per the COG?
5 factors used to classify NB in COG low-, intermediate-, and high-risk groups:
1. Stage, INSS
2. Age
3. N-myc status
4. DNA ploidy
5. Shimada classification
(Mnemonic: SANDS)
An NB pt with stage I Dz and n-myc amplification is in what risk group?
All stage I NB pts are low risk.
Can a pt with n-myc amplification be classified as intermediate risk?
No. All NB pts with n-myc are either low risk or high risk.
What makes a stage 2 or stage 3 pt high risk?
Stage 2 patients are high risk if they have all 3 risk factors: (1) n-myc amplification, (2) unfavorable histology, and (3) >1 yo.
Stage 3 patients need 1 risk factor to be high risk: either (1) n-myc amplification, or (2) both unfavorable histology ≥1 yo.
What feature makes NB pts with stage 4S Dz high risk?
NB stage 4S pts are high risk if tumors are n-myc amplified.
What features make NB pts with stage 4S Dz intermediate risk?
NB stage 4S pts are intermediate risk if tumors are not n-myc amplified and are either Shimada UH or have diploid DNA.
In which COG risk group do NB pts most commonly present?
NB pts are most commonly high risk (55%) → low risk (30%).
 TREATMENT/PROGNOSIS
TREATMENT/PROGNOSIS
Estimate the 3-yr OS for low-, intermediate-, and high-risk NB.
NB 3-yr OS by risk group:
Low risk: 95%–100%
Intermediate risk: 75%–98%
High risk: <30%
What percentage of stage 4S patients experience spontaneous regression?
Up to 85% of patients with stage 4S NB experience spontaneous regression. Thus, low-risk stage 4S patients can be observed.
What is the Tx paradigm for low-risk NB?
Low-risk NB Tx paradigm: surgery alone with chemo reserved for persistent or recurrent Dz
What is the Tx paradigm for low-risk stage 4S NB, and which study supports this approach?
Low-risk stage 4S NB Tx paradigm: Bx → supportive care. Chemo and/or RT are reserved for rapidly growing or symptomatic Dz. A subgroup analysis of CCG 3881 showed that supportive care is sufficient for 57% of pts. The protocol resulted in a 5-yr EFS of 86% and an OS of 92%. (Nickerson HJ et al., JCO 2000)
Which studies support the use of observation (without resection) in infants with localized NB without n-myc amplification?
The use of observation (without resection) in infants with localized NB without n-myc amplification was evaluated in the German GPOH trials NB95-S and NB97. Of 93 pts with gross Dz, 44 had spontaneous regression. OS and DM-free survival were no different from outcomes of pts treated with surgery or chemo in these trials (3-yr OS 99%, DM-free survival 94%). (Hero B et al., JCO 2008)
What is the role of RT in the Tx of intermediate-risk NB?
In intermediate-risk pts, RT is typically reserved for those who are symptomatic due to tumor bulk and are not responding to initial chemo, such as pts with respiratory distress due to hepatomegaly or with neurologic compromise due to cord compression. RT is not indicated as a consolidative therapy even with persistent Dz. Indications for RT based on A3961: Symptomatic palliation, viable residual Dz in Tx-refractory pts, and recurrent Dz.
What is the Tx for unfavorable stage 4S (intermediate-risk) Dz?
The Tx is chemo ×8 cycles.
What is the Tx paradigm for high-risk NB?
High-risk NB Tx paradigm: induction chemo, then resection, then high-dose chemo and stem cell transplant → consolidation RT, then oral cis-retinoic acid and immunotherapy (anti-GD2 + IL2/GM-CSF).
Which targeted agent has recently been demonstrated as promising new adj therapy for high-risk NB?
Promising results have been observed with immunotherapy targeting the surface glycolipid molecule disialoganglioside (GD2). A recent phase III randomized trial showed a significant improvement in event-free survival and OS for children with high-risk NB receiving chimeric anti-GD2 (ch14.18) combined with cytokines (IL2 and GM-CSF) and isotretinoin after myeloablative consolidation therapy. (Yu AL et al., NEJM 2010)
In low-risk and intermediate-risk NB, what dose of radiation is generally used?
In low-risk NB, radiation to 21 Gy at 1.5 Gy/fx can be used for Sx that do not respond to chemo. In intermediate-risk NB, if PR to chemo and viable residual disease after second-look surgery, then RT can be given locally to the primary + 2-cm margin to 24 Gy at 1.5 Gy/fx.
In high-risk NB, what tissues are targeted during RT and to what dose?
Per current COG0532, high-risk NB pts are treated with RT to their postchemo, preop tumor bed to a total dose of 21.6 Gy in 1.8 Gy/fx if GTR and 36.0 Gy (21.6 Gy to preop GTV → 14.4 Gy boost) if gross residual.
In high-risk NB, should elective nodal RT be given?
No. In high-risk NB, only clinically+ or pathologically+ LN regions are covered in the RT volumes.
What study indirectly demonstrated an RT dose response in high-risk NB?
Haas-Kogan et al. performed a secondary analysis of CCG 3891 and found that high-risk NB pts who rcvd 10 Gy local EBRT + 10 Gy total body irradiation (TBI) as part of a transplant preparation regimen had better LC than pts who did not get TBI (or a transplant) (5-yr LR rate was 22% vs. 52%). (IJROBP 2003)
These results support the current use of 21.6 Gy in high-risk protocols.
What study demonstrated the benefits of high-dose chemo → BMT as well as adj cis-retinoic acid in high-risk NB?
In CCG 3891, 379 high-risk NB pts were treated with induction chemo → surgery and 10 Gy to gross residual. Pts were then randomized to 3 cycles of nonmyeloablative chemo vs. myeloablative chemo, TBI, and BM T. Pts underwent secondary randomization to observation vs. cis-retinoic acid × 6 mos. Both the myeloablative chemo and cis-retinoic acid improved OS. 5-yr OS for pts who rcvd both was 59%. (Matthay KK et al., JCO 2009)
What is the appropriate Tx for NB pts with cord compression?
Consider chemo initially for NB-related cord compression. Unresponsive Dz can be treated with surgery or RT.
What is the RT dose and dose/fx used for NB pts being treated for symptomatic cord compression?
For symptomatic cord compression:
1. If pt is <3 yo, treat to 9 Gy (1.8 Gy/fx).
2. If pt is ≥3 yo, treat to 21.6 Gy (1.8 Gy/fx).
What is the RT dose and dose/fx used for NB pts being treated for symptomatic hepatomegaly?
Symptomatic hepatomegaly is treated to 4.5 Gy (1.5 Gy × 3).
Can the vertebral body be split during radiation planning?
No. It is necessary to always cover the full width of the vertebrae to avoid scoliosis.
What chemo drugs are typically used in NB?
Chemo drugs typically used in NB:
1. Cytoxan
2. Doxorubicin
3. Etoposide
4. Carboplatin
5. Ifosfamide
What is the role of I-131 MIBG in NB?
I-131 MIBG can be used for refractory NB, based on a promising phase II study showing a 36% response rate. (Matthay KK et al., JCO 2007)
 TOXICITY
TOXICITY
In NB, what dose constraint is used for the contralat kidney?
Limit the dose to the entire contralat kidney to <15 Gy.
In NB, what dose constraint is used for the liver?
Limit liver V15 to 66%.
In NB, what dose constraint is used for the lung?
Limit lung V15 to <66%.
What are some complications of radiation treatment in NB?
Disturbances of growth, infertility, neuropsychologic sequelae, endocrinopathies, cardiac effects, pulmonary effects, bladder dysfunction, secondary malignancy
Table 4.1 Children’s Oncology Group Risk Groupings
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


