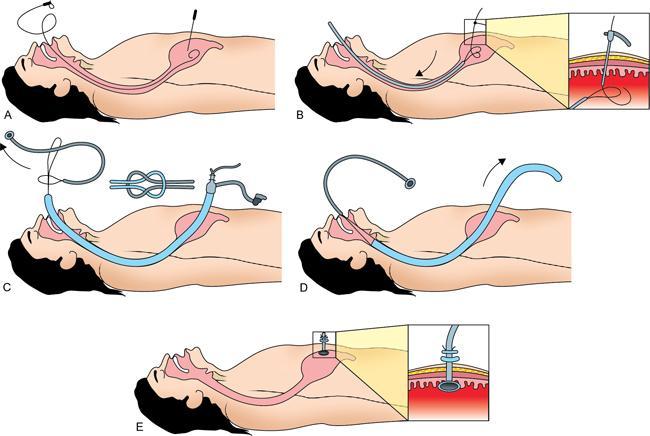
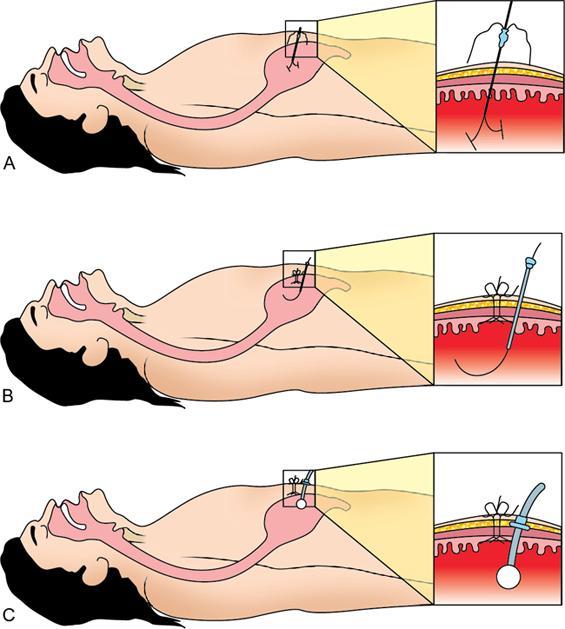
Arul AS Babu, Aswin Padmanabhan, Shyamkumar N. Keshava Certain diseases like motor neuron disease and stroke with bulbar palsy may render the patient unable to swallow and take nutrition orally. Providing good nutrition plays an important role in improving quality of life and longevity of patients who are bedridden with chronic illness. Nasogastric tubes placed are temporary arrangements as they have high chances of being displaced, getting occluded and causing significant discomfort. A gastrostomy tube placement for good nutrition has significantly longer survival time in comparison to Total Parenteral Nutrition (TPN). There are broadly three techniques of gastrostomy placement – radiological, endoscopic and surgical. Amongst these, radiological and endoscopic methods have not shown overall significant difference in outcome though certain clinical scenarios may obviate one technique over the other. Surgical technique of gastrostomy placement is usually reserved for patients as an add on when performing surgery for other reasons. In this chapter, we shall investigate radiologically inserted gastrostomy (RIG) techniques. Gastrostomy tubes are placed with long-term nutrition in mind and so a physical tube in the abdomen is inevitable. Patients and relatives need extensive counselling regarding the procedure and also maintenance of tube and a prior informed consent should be taken. RIG may be done by two techniques – Push-type gastrostomy Technique and Pull-type gastrostomy Technique. The choice of technique depends upon availability of oral access to the stomach. The gastrostomy tube requirements for pull technique and push technique are different. For pull-type, we use 24-Fr silicon tube of a PEG set for endoscopic use (PEG-24-PULL-S; Wilson-Cook Medical, Winston-Salem, USA). This tube consists of a mushroom catheter tip at the proximal end with inner and outer bolsters for fixation with tubing clamp. For push-type, Cope gastrointestinal suture anchor set (Cook, Bloomington, IN, USA) and 18-Fr silicon balloon catheter (ENTUIT Gastrostomy BR, Wilson-Cook Medical, Winston-Salem, USA). This technique is preferred when there is access to the stomach through the oral cavity, for example, Motor Neuron disease-associated dysphagia in which swallowing is the concern unlike oesophageal tumour when there is no access. A Nasogastric tube is placed at the outset and stomach is inflated with air until its shadow is clearly seen under fluoroscopy. The stomach is then percutaneously accessed with an 18 G needle. After placing a sheath, a wire and catheter is negotiated into the oral cavity through the GE junction. The gastrostomy tube is railroaded after exchange with an Amplatz stiff wire. After pulling the tube out through the gastrostomy opening, it is fixed with the help of a button which comes in the package (Fig. 7.18.1). This technique is used when access to stomach through the oropharyngeal route is not possible. In this technique, stomach is punctured using specialized introducer needle preloaded with anchors which have threads attached to them. Once the anchor is in place, they are thread from the anchor is tied on the anterior abdominal wall. This step brings the stomach close to the anterior wall and is called gastropexy. Further, another puncture is made just next to the gastropexy needle with a 18 G needle. After serial dilatation over the wire, a push-type gastrostomy tube is placed through this opening (Fig. 7.18.2). Percutaneous gastrostomy is an important step toward treatment of patients with chronic illnesses who cannot take oral feeds. Radiologically guided gastrostomy tube placement is one of the three techniques for placing gastrostomy tubes. Attention to detail and meticulous technique will help improve outcome and reduce complications of the procedure. Intraluminal balloon dilatation and stenting of the gastrointestinal tract are performed to relieve gastrointestinal obstruction caused by benign/malignant pathologies. In principle, they are similar to angioplasty and stenting of the blood vessels in that the procedure involves accessing the lumen, safely crossing the obstructive lesion, balloon dilatation and stenting. Intraluminal procedures using fluoroscopic guidance are generally limited to the oesophagus, stomach, pyloroduodenal junction and colon. Oesophagus Oesophageal balloon dilatation Oesophageal stenting Stomach/duodenum Colon There are no absolute contraindications, the relative contraindications are: Oesophagus Gastric/duodenal Colon Upper GI Series: For oesophagus, gastric and duodenal procedures to evaluate extent and appearance (benign/malignant) of stricture.Contrast Enema: For preprocedure evaluation of colonic lesions to assess extent and appearance. Look for presence of fistulas. CT: Useful to evaluate extraluminal pathology, extrinsic compression, presence of distal small bowel obstruction, presence of peritonitis and pneumoperitoneum. Endoscopy/colonoscopy whenever possible can help in assessing extent of lesion and obstruction, apart from obtaining tissue sample for histopathological evaluation. Platelet count, Prothrombin time with INR (International Normalized ratio) should be checked for all patients. For those who present with symptoms of obstruction, electrolyte imbalance should be ruled out prior to procedure. Oesophageal and Gastroduodenal Procedures: The oral cavity is anaesthetized with lidocaine spray and a 4F catheter with guidewire is negotiated into the oral cavity up to the level of obstruction. The guidewire is removed and contrast is instilled under fluoroscopy to confirm intraluminal position of catheter and assess extent of stricture. The stricture is then crossed with catheter-guidewire manipulation. The guidewire is exchanged for a stiffer Amplatz wire. The stent delivery system is advanced over the Amplatz wire and stent is deployed. The stent is sized such that it has a proximal and distal landing zone of 2 cm within the normal lumen. If only balloon dilatation is intended, the balloon is tracked over the Amplatz wire and slow, sustained balloon inflation is performed to obtain luminal dilatation. Post balloon plasty/stenting contrast instillation is performed to ensure lumen patency and exclude complications. Colonic procedures: Similar to oesophageal procedures the colon is accessed through the anus with catheter and guidewire, the obstructive lesion is crossed and balloon dilatation or stenting is done over a stiff guidewire.
7.18: Nonvascular interventions in the abdomen
Percutaneous gastrostomy
Introduction
Indications
Contraindications
Patient preparation
Technique and material required
Pull-type gastrostomy technique
Push-type gastrostomy technique
Postprocedure care and follow-up
Complications
Conclusion
Balloon dilatation and stenting for bowel obstruction
Introduction
Indications
Contraindications
General
Preprocedure evaluation
Imaging
Laboratory parameters
Procedure
Equipment required
Anaesthesia
Technique
Postprocedure care
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


