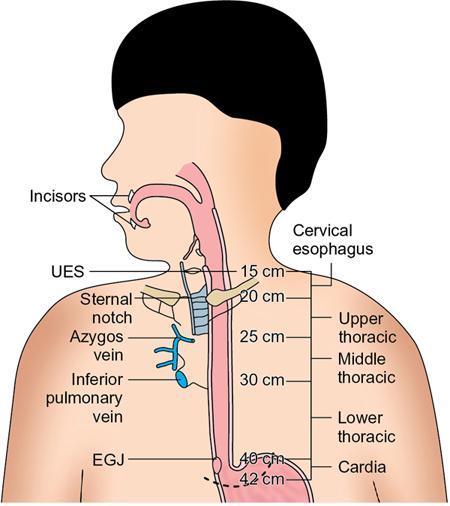
• Oesophagus is a fibromuscular tube that extends from crico-pharynx to gastro-oesophagal (GE) junction. It is divided into four parts according to the AJCC classification system (Fig. 7.3.1). These parts are well seen on coronal images of CT.
• Cervical oesophagus
• Thoracic oesophagus
• Abdominal oesophagus
Anatomical name
Anatomical Extension
Cervical
Hypopharynx to sternal notch
Thoracic-upper
Sternal notch to azygos vein
Thoracic-middle
Lower border of azygos vein to inferior pulmonary vein
Thoracic-lower
Lower border of inferior pulmonary vein to EGJ
Abdominal
EGJ to 2 cm below EGJ
EGJ, esophagogastric junction.
• Normal oesophageal features on barium studies
• In most patients, normal mucosal surface is smooth and featureless.
• Normal longitudinal folds are seen in partially collapsed oesophagus – measuring 1–3 mm in thickness.
• Occasionally transverse folds may be seen in normal patients.
• At the junction of smooth and striated muscle in midthoracic oesophagus (at the level of aortic arch) – spiculated transverse fold may be seen and is a normal finding.
• Normal external impression on oesophagus
• Aortic arch
• Left main bronchus
• Heart
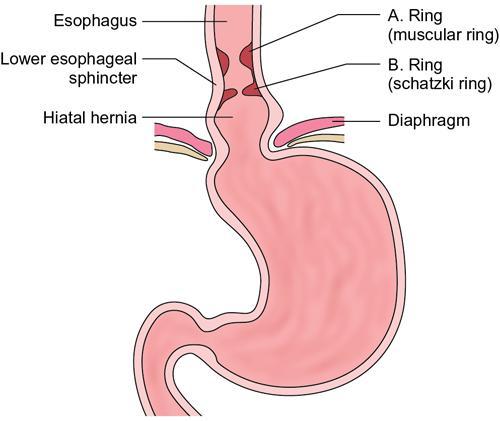
• Oesophageal rings and Oesophageal vestibule (Fig. 7.3.2)
• A ring/Wolf ring –
• It is the muscular contraction at the junction of tubular oesophagus and vestibule.
• It has no definite anatomic correlate.
• B ring –
• It is normally seen located at squamocolumnar junction (Z line). The appearance does not change during the examination.
• Significance:
• If the B ring is >20 mm wide, no obstruction occurs.
• If the B ring is 13–20 mm wide, it may cause episodic dysphagia, and is then called a SCHATZKI RING.
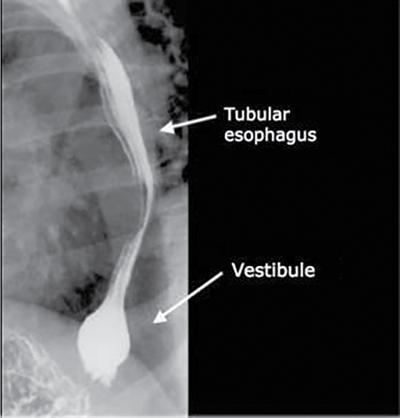
• Between the A and the B rings the distal oesophagus enlarges and becomes fusiform – known as phrenic ampulla or oesophageal vestibule.
• Bulbous distension of distal 2–4 cm of lower oesophagus is called vestibule and corresponds to the manometrically defined high-pressure zone that constitutes the lower oesophageal sphincter.
• It is best demonstrated by breath-holding in inspiration or Valsalva manoeuvre.
• Refers to idiopathic thickening of gastric pyloric musculature which then results in progressive gastric outlet obstruction.
• Seen in newborn babies as early as 3 weeks.
• Measurements are made of thickened hypoechoic pylorus on ultrasound (US). Gallbladder is identified on US and probe is turned obliquely sagittal to the body to visualize the pylorus.
• Anterior displacement of the abdominal viscera in barium studies is an indirect sign of a retroperitoneal tumour/mass. It was first described by Brown in 1928. Subsequently, detailed study in measurement of retrogastric space was conducted by Poppel, Schinmel and Mednick. This was further researched by Schultz in 1958 and 1965 and subsequently by Poole in 1972.
a. Grossly, the width of this space (measured where stomach crosses the midline) in a supine patient should not exceed that of the subjacent vertebral body. However, it can be increased in obesity and with ascites (Fig. 7.3.10).
b. Schultz described the normal ranges by employing right lateral recumbent view and left lateral erect view. The patients have to be classified as hyposthenic, sthenic and hypersthenic depending on the AP diameter measured with calipers.
Only gold members can continue reading. Log In or Register to continue