CHAPTER 85 Nuclear Medicine
Extrathoracic Vascular Imaging
Compared with catheter angiography, CT angiography, and MR angiography, nuclear medicine is a small component of extrathoracic vascular imaging. This component is crucial, however; the specific questions answered safely and efficiently by nuclear medicine cannot be answered by any other modality. Historically, radioisotope techniques have been used widely to answer research and clinical vascular questions. Some early nuclear angiographic procedures contributed greatly to our knowledge of cardiac and vascular physiology and diagnosis of various peripheral vascular disorders.1 These techniques capitalize on the ability of noninvasive radioisotope imaging to depict existing physiologic parameters accurately without changing the physiology being interrogated.
Bleeding studies benefit from dynamic cine sequences, which show in rapid succession multiple images acquired at short intervals (Fig. 85-1). This sequence of images gives the interpreting physician greater confidence in localizing a bleeding site or visualizing the progressive accumulation of activity in a Meckel diverticulum (Fig. 85-2). Brain SPECT studies have benefited from advances in software allowing digital image fusion of the radioisotope study with CT or MRI anatomic sectional images, further computer comparison with probabilistic brain atlases, and three-dimensional volume rendering.

 FIGURE 85-1
FIGURE 85-1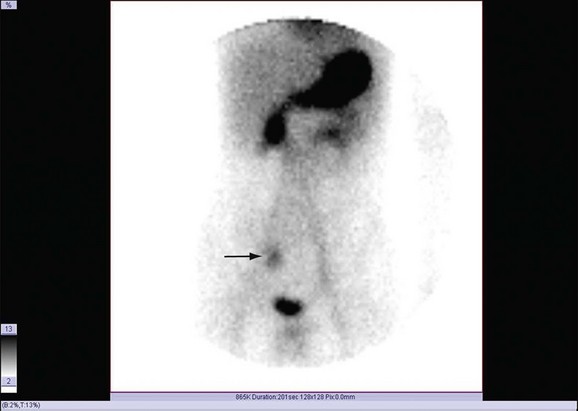
 FIGURE 85-2
FIGURE 85-2Nuclear medicine continues to refine its preexisting role in extrathoracic cardiac imaging even as it expands to assess atherosclerosis with positron emission tomography with 18FDG. This study is still in its experimental phase, but shows great promise as an imaging adjunct.2
GASTROINTESTINAL BLEED LOCALIZATION SCAN
Technique Description
No specific patient preparation is required for a Tc 99m–radiolabeled erythrocyte scan. This is an advantage because studies for gastrointestinal bleeding are usually requested emergently. Various labeling methods and kits are available to label the red blood cell, including an in vitro method, an in vivo method, and a hybrid method. The in vitro method using widely available kits typically provides very high labeling efficiency (e.g., Ultratag kit [Mallinckrodt, Inc., St. Louis]) provides a labeling efficiency of 98.5%).3 What the methods have in common is the use of stannous ion as a reducing agent and the Tc 99m label.
The patient is positioned supine with the camera located anteriorly. On initial intravenous injection of the radiolabeled erythrocytes, initial flow images are obtained at 1 s/frame for 60 frames. Subsequent dynamic images are obtained at 1 min/frame for 60 additional frames. A 128 × 128 image matrix is normally used for both acquisitions.4 Additional imaging may be repeated at intervals up to 24 hours, but all acquisitions should be in a dynamic series to enable detection of subtle bleeding sites and peristaltic transit through the bowel.
Pitfalls and Solutions
The most common technical pitfall of the Tc 99m–radiolabeled erythrocyte scan relates to an imperfect tagging of the blood cells, leaving free Tc 99m pertechnetate in the bloodstream. As described earlier, tagging efficiency is typically very high, especially with the in vitro technique. Common drugs such as heparin, penicillin, and iodinated contrast media interfere with the entry of the reducing agent (Sn++) through the red blood cell membrane, however, causing an increased amount of free pertechnetate in the blood.5 Also, alternative in vivo labeling techniques may allow a certain amount of free pertechnetate to circulate.
Free pertechnetate appears in the stomach where it is physiologically secreted by the gastric parietal cells (see Fig. 85-2). This activity has an intraluminal configuration and moves antegrade over time. This movement can simulate an upper gastrointestinal bleed. In some instances, an upper gastrointestinal bleed may have been ruled out from a recent endoscopy, or the clinical presentation may not be consistent with one. A static image of the neck also reveals physiologic uptake of pertechnetate in the thyroid gland. After confirmation of the presence of free pertechnetate, the best solution is to allow for it in the interpretation. A brisk lower gastrointestinal bleed should be differentiated easily on dynamic imaging.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


