| SKULL BASE REGION | Left sella turcica and left cavernous sinus |
| HISTOPATHOLOGY | Nonfunctioning pituitary macroadenoma |
| PRIOR SURGICAL RESECTION | Yes |
| PERTINENT LABORATORY FINDINGS | All pituitary labs within normal limits |
Case description
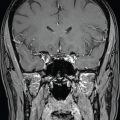
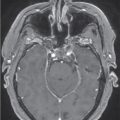
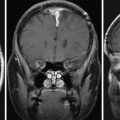
A 61-year-old woman was diagnosed with an incidental pituitary mass during a workup for fatigue. She was not treated at the time and did not develop symptoms until 16 years later when she underwent ophthalmologic evaluation for abnormal vision in her left eye. Formal visual field tests revealed a left temporal deficit, and MRI imaging showed significant growth of the sellar mass with suprasellar extension, bilateral cavernous sinus invasion (left greater than right), chiasmal compression, and extension into the sphenoid sinus and nasopharynx ( Figure 3.11.1 ). The tumor measured 39 × 40 × 50 mm. Pituitary hormone levels were within normal limits. The patient underwent near-total endonasal transsphenoidal resection, which was complicated by a cerebrospinal fluid leak and managed with lumbar drain placement. A small residual mass remained in the left cavernous sinus ( Figure 3.11.2 ). Pathology revealed a null-cell pituitary adenoma, immunonegative for hormones. A 2-month postoperative follow-up with her ophthalmologist showed improvement in her visual field deficits without complete resolution.


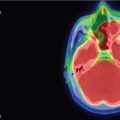
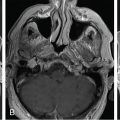
Three months after the resection, the patient started experiencing cold intolerance, and her T4 was found to be low at 0.5 ng/dL. She was started on daily levothyroxine 0.075 mg and had resolution of her symptoms with subsequently normal endocrine lab values. Follow-up imaging showed a stable residual tumor until 3 years after the initial resection. MRI at this time showed an increase in the portion around the left carotid artery ( Figure 3.11.3 ). She was referred for Gamma Knife Radiosurgery (GKRS) of the residual tumor ( Figure 3.11.4 ).
| Radiosurgery Machine | Gamma knife |
| Radiosurgery Dose (Gy) | 16, at 50% isodose line |
| Number of Fractions | 1 |
Related posts:
 Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
 ACTH secreting – delayed postoperative radiosurgery of gland for recurrent pathology-negative cushing disease
ACTH secreting – delayed postoperative radiosurgery of gland for recurrent pathology-negative cushing disease
 Chordoma – immediate postoperative/post-proton therapy radiosurgery for residual disease
Chordoma – immediate postoperative/post-proton therapy radiosurgery for residual disease
 Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
 Capillary hemangioma – postoperative radiosurgery for residual tumor
Capillary hemangioma – postoperative radiosurgery for residual tumor
 Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


