(1)
Department of Clinical Radiology, Amiri Hospital – Kuwait City, Kuwait City, Kuwait
12.1 Medications Toxicity
12.1.1 Antibiotics
12.1.3 Methotrexate
12.1.4 Hypervitaminosis A
12.1.5 Anticonvulsants
12.1.6 Amiodarone Toxicity
12.1.7 Cyclosporine A
12.1.8 Glucocorticoids
12.2 Drugs of Abuse
12.2.1 Cocaine and Heroin (Opioids)
12.2.2 Alcohol
12.2.3 Toluene Toxicity
12.2.4 Methanol Toxicity
12.2.5 Amphetamines Abuse
12.2.6 Marijuana
12.2.7 Butane Poisoning
12.3.1 Arsenic Poisoning
12.3.2 Mercury Poisoning
12.3.4 Pneumoconiosis
12.3.6 Carbon Monoxide Poisoning
12.3.7 Manganese Poisoning
12.3.9 Methyl Bromide Poisoning
12.3.10 Tattoos
12.4.2 Cyanide Poisoning
12.4.3 Botulism
12.1 Medications Toxicity
Toxicology is the study of the harmful effects of drugs, organic substances, and medication on the human body. Many medications and substance abuse can result in radiologic manifestations during imaging patients for a variety of conditions. Knowledge of the radiological signs of certain common medications and abused substances helps radiologists in the interpretation of these radiological abnormalities and artifacts when encountered incidentally. In this topic, selected medications and drugs which have well-recognized radiological signs are discussed and illustrated
Antibiotics
Antibiotics abuse can kill the normal flora and cause pseudomembranous colitis in long-term use. Pseudomembranous colitis is a disease characterized by overgrowth of the organism Clostridium difficile, a colonic bacterium living as a part of the normal flora. The bacteria produce toxins that injure the intestinal mucosa and form a covering layer of exudates and necrotic cells from the intestinal mucosa; this layer impedes the intestinal absorption and leads to watery diarrhea. Pseudomembranous colitis may occur also with chemotherapy, abdominal surgery, and hypotensive episodes. Diagnosis is established by stool assay for C. difficile.
Signs on CT
- 1.
The most common sign of pseudomembranous colitis is circumferential or eccentric thickening of the colonic wall, typically more than 15 mm, while the normal colonic wall thickness in CT is 3 mm (accordion sign) (Fig. 12.1.1). This sign however is not specific for pseudomembranous colitis, but characteristic.
- 2.
Although colonic wall thickening can be seen in many inflammatory diseases, the colonic wall thickening in pseudomembranous colitis is generally greater than any other inflammatory disease.

Fig. 12.1.1
Axial (a) and coronal (b) CT images of a 72-year-old patient admitted to the hospital with repeated vomiting, weight loss, and watery diarrhea since 10 days, and she was treated with intravenous antibiotics for 5 days prior to the CT. The CT showed diffuse, concentric wall thickening (15.5 mm max) with diffuse haustral thickening (accordion sign; arrow) of the whole colon, characteristic of acute diffuse colitis (pseudomembranous colitis in conjunction with history of antibiotic use)
Metformin (Glucophage, Oral Hypoglycemics)
Diabetes mellitus is treated with oral hypoglycemics and insulin, depending of the type of diabetes. The most commonly used oral hypoglycemic medications groups are sulfonylureas and biguanides.
Sulfonylureas are medications that increase insulin secretion and reduce peripheral resistance to insulin. An example of a sulfonylurea drug is gliclazide (Diamicron). Sulfonylureas causes inhibition of adenosine triphosphate (ATP)-sensitive potassium channels on the membrane of pancreatic beta cells, augmenting depolarization of the cell and enhancing the release of endogenous insulin. The main side effects of sulfonylureas include prolonged or recurrent hypoglycemia and weight gain.
Biguanides are medications that reduce glucose absorption, inhibit gluconeogenesis, and increase peripheral glucose utilization. An example of a biguanides drug is metformin (Glucophage). The main side effects of biguanides include gastrointestinal (GI) symptoms, anorexia, lactic acidosis, and maybe megaloblastic anemia. The GI symptoms of metformin include diarrhea, epigastric pain, and gastroparesis. Prolonged gastroparesis may predispose to the formation of gastric bezoars. Gastric bezoar is a rare condition characterized by foreign body mass formation within the stomach usually due to accumulation of indigested material in the form of masses or concretions. It usually forms from vegetable, fruits, or hair (in psychiatric patients) in patients with gastric emptying problems.
Methotrexate
Methotrexate is a folate (vitamin B9)-antagonist used in the treatment of many malignant and inflammatory conditions such as leukemia, sarcomas, breast carcinoma, rheumatoid arthritis, and psoriasis. Routs of administration include oral, intravenous, intramuscular, and intrathecal routs.
Methotrexate toxicity is known to cause lung symptoms that include cough and dyspnea, fever, chills, malaise, and headache weeks after initiation of therapy. Other manifestations include peripheral eosinophilia (50 %), skin rash (17 %), pleural effusion, pulmonary fibrosis, hepatic steatosis, malabsorption and diarrhea, and hilar lymphadenopathy
Methotrexate lung-related changes may present with two rare manifestations: acute pleuritis (pleural chest pain with pleural effusion) or acute respiratory failure secondary to noncardiogenic edema (acute respiratory distress syndrome).
Methotrexate can induce diffuse white matter lesions with demyelination and necrosis (leukoencephalopathy). Disseminated necrotizing leukoencephalopathy is a rare condition characterized by bilaterally symmetrical necrosis of the thalami and maybe other basal ganglia. Histopathologic features include multifocal, coalescing areas of coagulative necrosis with axonal swelling in the periventricular white matter.
Signs on Radiographs
- 1.
Noncardiogenic edema can be seen as bilateral diffuse alveolar shadows with normal-sized heart, typically starting from the periphery to the center. Pleural effusion with bilateral hilar lymphadenopathy may be seen.
- 2.
Other rare pulmonary manifestation includes noncaseating granulomas. Pulmonary fibrosis may arise in chronic use.
- 3.
Methotrexate can cause profound osteoporosis that can cause multiple insufficiency fractures.
- 4.
Methotrexate use in children and adolescent may cause growth recovery lines (Harris lines). Harris lines are radiodense transverse lines that run parallel to the epiphyseal scar in the metaphysis (Fig. 12.1.2). They represent periods of increased bone growth followed by periods of suppressed bone growth. These lines are usually seen in the distal femur or the proximal tibia. They are considered as normal variants in asymptomatic patients or patients without history of medication use. These lines must not be mistaken with stress fractures.
- 5.
Other musculoskeletal features include metaphyseal corner fracture and ring epiphyses. These changes can be seen within 2 months after starting therapy.

Fig. 12.1.2
Lateral plain radiograph of the knee that demonstrates Harris lines (arrowheads)
Signs on US
Hepatic steatosis can be seen in long-term methotrexate use due to liver drug detoxifying injury.
Signs on MRI
Acute necrotizing encephalopathy is classically seen as bilateral symmetrical thalamic high signal intensity lesions seen on T1W images with mixed high/low T2 signal intensity lesions due to necrosis and hemorrhage. DWI shows decreased signal in ADC map due to cytotoxic edema and hemorrhage. No contrast enhancement is typically seen (due to ischemic nature of the injurious insult).
Hypervitaminosis A
Vitamin A is a fat-soluble vitamin primarily found in fish liver (retinol) and carrots (β–carotene). Vitamin A contains retinol esters; when the liver is saturated with vitamin A, retinol esters appear in the blood in toxic levels, causing different systemic manifestations.
Hypervitaminosis A is often seen in children and young adults treated with high doses of vitamin A (>100,000 IU per day). Also, vitamin A derivatives use during pregnancy can induce teratogenic effect (induce fetal malformations). Moreover, vitamin A can cause premature closure of the epiphyses in humans. The same condition can occur in calves, causing premature closure of their hind limb making their gait resemble that of hyena, a disease of calves known as Hyena disease.
Hypervitaminosis A targets mainly the central nervous system (fatigue, irritability, hypersomnia, anorexia, and increased intracranial pressure and pseudotumor cerebri in children), liver (liver cirrhosis, jaundice, and hepatomegaly), skin (alopecia and skin peeling), mucous membranes (cheilitis and stomatitis), and musculoskeletal system (bone pain and unexplained swelling of extremities). Diagnosis is confirmed by detecting high serum levels of retinol esters (>100 μg/dL). Radiologically, hypervitaminosis A causes diaphyseal periosteal reaction, which can mimics battered child syndrome.
Battered child syndrome (child abuse) refers to injuries sustained by a child as a result of physical abuse. The physical signs are arranged from internal injuries, cuts, burns or fractured bones. Shaken baby syndrome is another form of child abuse where the infant or the child presents with retinal hemorrhage, subdural or subarachnoid hemorrhage, with absence of external signs of physical abuse. It occurs due to shaking force inflicted to the baby by the abuser.
Signs on Radiographs
- 1.
Classically, chronic hypervitaminosis A shows osteoporosis, premature closure of physis, periosteal reaction, and cortical hyperostosis of the cranium and long bones. The periosteal reaction observed in long bones may mimic that reaction of Ewing’s sarcoma, especially in young adults.
- 2.
Typically, periosteal reaction due to vitamin A toxicity is seen in the diaphysis of the ulna and the metacarpals. Other sites affected include clavicles, tibia, and fibula.
- 3.
Cervical osteophytes, syndesmophytes, and changes similar to ossification of posterior longitudinal ligament can be seen in long-term use of retinoic acid (vitamin A derivative), which is used to treat acne.
- 4.
Battered child syndrome can be suspected radiologically by finding the following radiographic manifestations: cortical thickening without fractures or dislocations; metaphyseal fragments at the area where the periosteum joins the metaphysis in long bones due to old periosteal hematoma; single or multiple transverse fractures in the long bones, ribs, or humerus with different healing stages (highly suspicious for child abuse); diaphyseal spiral fractures, they result from twisting or torsion forces (highly indicative of child abuse); and scapular fractures in babies (highly indicative for child abuse).
Signs on CT and MRI
- 1.
In hypervitaminosis A, sutural diathesis and hyperostosis in association with signs of intracranial pressure and ventriculomegaly may be seen due to altered cerebrospinal fluid mechanics.
- 2.
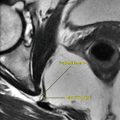
In shaken baby syndrome, unilateral or bilateral subdural hematomas are typically seen with signs of acute on top of old subdural hematoma may be seen due to recurrent abuse (Fig. 12.1.3).

Fig. 12.1.3
Axial T* (a) and time-to-flight (TOF) angiographic MR images of an infant with bilateral subdural hematomas (arrowheads) due to child abuse (shaken baby syndrome); the infant stayed in the pediatric intensive care unit for 5 weeks before she died
Anticonvulsants
Anticonvulsants are medications that prevent seizure incidence by raising seizure threshold or decrease the activity of epileptogenic foci in the brain. Most anticonvulsants act by decreasing levels of excitation neurotransmitters (e.g., glutamate) and increasing inhibitory neurotransmitters (e.g., gamma–aminobutyric acid/GABA). Examples of anticonvulsants include:
- 1.
Carbamazepine: it decreases neuronal excitation by prolonging sodium (Na+) channel activation. Carbamazepine toxicity includes cardiac toxicity, stupor, encephalopathy, and chorea. Fetal carbamazepine syndrome is a pathological condition that affects neonates in mothers treated with carbamazepine during pregnancy; features include nail hypoplasia, spinal dysraphism, congenital heart disease, microcephaly, tall forehead, malar hypoplasia, and micrognathia.
- 2.
Phenytoin: like carbamazepine, it decreases neuronal excitation by prolonging sodium channels (Na+) channel activation. Phenytoin toxicity includes cardiac toxicity (intravenous phenytoin mainly), gingival hyperplasia, ataxia, nystagmus, chorea, ophthalmoplegia, hypotension, and hirsutism. Phenytoin can cause immunodeficiency in children treated with phenytoin and infected with Epstein–Barr virus. Fetal phenytoin syndrome is a pathological condition that affects neonates in mothers treated with phenytoin during pregnancy; features include dwarfism, hypoplastic phalanges, nail hypoplasia, frontal bossing, tall forehead, maxillary hypoplasia, hirsutism, and microcephaly. Phenytoin can induce hypersensitivity syndrome characterized by lymphadenopathy and patchy alveolar infiltrations similar to Loeffler endocarditis. Lymphadenopathy due to phenytoin use is classified into four main categories: lymphatic hyperplasia, lymphatic hyperplasia that regresses after discontinuing the therapy (pseudolymphoma), lymphatic hyperplasia that regresses after discontinuing the therapy and then reemerge several months after (pseudopseudolymphoma), and true lymphoma (Hodgkin’s or non–Hodgkin’s lymphoma).
- 3.
Valproic acid: it decreases neuronal excitation by prolonging sodium channels (Na+) channel activation and increase GABA activity. Valproic acid toxicity can cause cardiac arrest in large doses, nausea, vomiting, cerebral edema, and rarely pancreatitis. Fetal valproate syndrome is a pathological condition that affects neonates in mothers treated with valproic acid during pregnancy; features include limb defects, spinal dysraphism, genital anomalies, cardiac anomalies, craniosynostosis (trigonocephaly), and tall forehead.
Signs on Radiographs
- 1.
Up to one third of patients on phenytoin may show signs of osteopenia due to reduced calcium absorption from the intestines. Also, it can cause dental root abnormality and thickening of the diploic space (similar to acromegaly).
- 2.
Phenytoin can cause thickening of the heel pad similar to that of acromegaly. On lateral plain radiographs, the soft-tissue density of the heel pad is >35 mm in diameter.
- 3.
Patchy alveolar infiltrations with hilar lymphadenopathy may be seen rarely on chest radiographs due to hypersensitivity syndrome induced by phenytoin.
Amiodarone Toxicity
Amiodarone is a class III antiarrhythmic agent used to control atrial and/or ventricular arrhythmia. Amiodarone is known to cause long-term complications that include pulmonary, endocrinal, ophthalmic, and hepatic manifestations.
Amiodarone can induce pulmonary toxicity found in the alveoli and the interstitial septae, inducing inflammatory reaction and fibrosis (13 % of patients using amiodarone). Patients present with nonspecific symptoms like fever, weight loss, cough, and dyspnea. The mechanism of amiodarone-induced pulmonary toxicity is presumed to be related to hypersensitivity pneumonitis or direct toxicity related to production of free radicals and phospholipidosis.
Amiodarone contains significant amount of iodine (37 % of its molecular weight), which can induce hyper- or hypothyroidism in patients using amiodarone (14–18 % of patients). The mechanism of amiodarone-induced hypothyroidism is thought to result from abnormal response of the thyroid to chronic high iodine load and then inability to resume normal thyroid function from the inhibitory effect of iodine uptake and hormone synthesis (Wolff–Chaikoff effect).
Amiodarone optic neuropathy is a very rare complication of amiodarone (0.36–2 % of patients using amiodarone for 5 years interval), and it mimics idiopathic anterior ischemic optic neuropathy (incidence is 0.3 % of population). Idiopathic anterior ischemic optic neuropathy is typically unilateral with visual loss that is not completely reversible. In contrast, amiodarone optic neuropathy is typically bilateral (key feature of toxicity) and visual loss is completely reversible when the drug is discontinued. Amiodarone also can cause corneal microdeposits that can cause visual loss or blurry vision (10 % of patients).
Amiodarone hepatic toxicity has an incidence of 1 % in patients using amiodarone and is referred to as hepatic phospholipidosis. Hepatic phospholipidosis, also known as pseudoalcoholic liver disease, is a condition characterized by accumulation of cytoplasmic phospholipid inclusions within macrophages, hepatic cells, and all body tissues as a cytotoxic effect of amiodarone and its metabolite desethylamiodarone. Liver histological characteristics of hepatic phospholipidosis include steatosis, necrosis, and cirrhosis. Patients may present with signs of hepatic liver dysfunction and hepatomegaly, with mild liver enzymes elevation.
Other manifestations of amiodarone toxicity include cutaneous photosensitivity, skin discoloration, vomiting, anorexia, and peripheral neuropathy.
Signs on US
Hepatic phospholipidosis is detected as highly echogenic liver due to steatosis, with or without signs of cirrhosis.
Signs on Radiographs
Amiodarone causes nonspecific patchy alveolar infiltrations, linear interstitial patterns, and reticular interstitial pattern due to fibrosing alveolitis.
Signs on CT
- 1.
In lung HRCT, nonspecific features can be seen and include high-attenuation lung masses (e.g., 86–174 HU), pulmonary alveolar patchy infiltrations, thickening of the interstitial septae, pleural effusion, and subpleural high-attenuation deposits (Fig. 12.1.4).
- 2.
Hepatic phospholipidosis is typically detected as low-density liver due to steatosis, with or without signs of cirrhosis. Hepatomegaly may be seen.

Fig. 12.1.4
Posteroanterior chest radiograph (a) and axial pulmonary HRCT (b) of a patient with chronic amiodarone use shows extensive, patchy, lobular reticulo-interstitial lung disease reflecting “amiodarone-induced pulmonary fibrosis”
Cyclosporine A
Cyclosporine A is a fungal metabolite that has the property of specifically and irreversibly inhibiting the induction of the cytotoxic effector and helper T cells without direct lymphocytotoxicity. It is one of the most commonly used drugs for transplantation rejection after steroids. Complications of cyclosporine include formation of pulmonary nodules (rarely), lymphadenopathy, hallucinations, and posttransplant lymphoproliferative disorder.
Posttransplant lymphoproliferative disorder (PTLD) has two different manifestation patterns: early and late. Early PTLD occurs within the 1st year after transplantation and is likely to regress after reduction in immunotherapy and less likely to result in disseminated lymphoma. Late PTLD, on the other hand, arises after 1 year posttransplantation and is associated with mortality in 70 % of cases due to disseminated lymphoma.
Signs on MRI
- 1.
Cyclosporine A toxicity causes reversible posterior leukoencephalopathy, which is seen as bilateral symmetrical occipital vasogenic edema that resolves when the drug is continued.
- 2.
Abnormal high T2 signal intensity with contrast enhancement affecting the parietal cortex bilaterally has been reported in the literature to occur with cyclosporine toxicity.
Glucocorticoids
Glucocorticoids are widely used, hormonal anti-inflammatory medications with wide adverse reactions. Glucocorticoids can induce pseudo-Cushing’s disease features such as obesity, hirsutism, osteoporosis, avascular necrosis (due to fat emboli), lipomatosis, hypercalciuria, and nephrolithiasis.
Signs on Radiographs
- 1.
Bone osteoporosis is a well-known feature of long-term glucocorticoids use. The etiology of osteopenia is thought to be secondary to inhibition of osteoblastic activity and the effects of increased levels of parathyroid hormone, and negative nitrogen balance and loss of proteinaceous matrix of the bone.
- 2.
Nephrocalcinosis is seen as patchy areas of calcifications at the renal shadows region on plain abdominal radiographs.
- 3.
Avascular necrosis is detected through increased bone density (due to ischemia which will affect the osteoclastic activity), subchondral lucency (late finding), and maybe collapse of the articular surface.
Signs on CT
Lipomatosis is seen as noncapsulated proliferation of fatty tissues. Classically, glucocorticoids-induced lipomatosis can be seen within the mediastinum, abdomen, or pelvis.
Signs on MRI
Avascular bone necrosis can be diagnosed early on MRI. Classically on post-contrast images, there is an outer low intensity line with an inner high intensity line seen in T2W sequence surrounding an area of low T1 and high T2 signal intensity within the affected epiphysis (double shadow sign). The high intensity line is believed to be caused by the zone of hyperemia. Double line sign is found in 80 % of cases of avascular necrosis.
Gadolinium-Based Contrast Media
Nephrogenic systemic fibrosis (NSF) is an idiopathic, progressive systemic fibrosis that arises in patients with renal disease. Gadolinium (Gd)-based contrast media are responsible for development of NSF in renal disease patients performing contrast-enhanced MRI.
The clinical manifestations of NSF is divided into acute (<2 weeks after contrast exposure) and chronic (>2 weeks after contrast exposure). The early manifestations include limb pain (52 %), followed by pruritus (36 %), alopecia, swelling (25 %) of the hands and feet, paresthesias (24 %), burning skin sensation (16 %), abdominal pain, and diarrhea. The chronic manifestations include bilateral symmetrical plaques (58 %), papules (32 %), or nodules (17 %) of cutaneous and muscle hardening (mimicking scleroderma), with brownish hyperpigmentation involving predominantly the lower extremities (41 %). Other features include joint stiffness (34 %) and skin tightness (30 %). The arms and trunk are less frequently involved, and rarely yellowish scleral plaques formation has been reported.
NSF has been reported in association with gadodiamide (Omniscan, GE Healthcare), gadopentetate (Magnevist, Bayer Healthcare), gadoversetamide (OptiMARK, Mallinckrodt Inc.), and gadoterate meglumine (Dotarem – Guerbet SA). The United States Food and Drug Administration (FDA) issued a warning in June 2006 against the use of Gd-contrast in patients with moderate-to-severe reduction in glomerular filtration rate (<30 ml/min) and patients who have undergone liver transplantation. Also, the FDA warned that the use of 0.2–0.3 mmol/kg even in a single exposure carry a high risk of NSF development in patients with compromised glomerular filtration rate.
The definitive diagnosis of NSF is made by deep skin biopsy, which typically should include the entire dermis and subcutaneous fat to the level of the fascia, if possible. Histology shows extensive dermal fibrosis, with alteration of the normal pattern of collagen bundles with surrounding clefts and increased number of spindle cells which typically stain positive for CD34 and procollagen-1 surface markers.
Signs on Radiographs
Patients with chronic NSF may show diffuse osteopenia, joint contractures, and extensive intra- and periarticular soft-tissue calcification.
Signs on CT and MRI
- 1.
Dural fibrosis with calcification has been reported to occur rarely in patients with chronic NSF in the presence of normal serum phosphorus levels.
- 2.
Diffuse dural thickening and enhancement may be seen.
Selected References
Brunner D, et al. CT of pseudomembranous colitis. Gastrointest Radiol. 1984;9:73–5.
Change PSM, et al. Amiodarone-induced hypothyroidism with EPO-resistant anemia in a patient with chronic renal failure. J Chin Med Assoc. 2008;71(11):576–8.
Chao CC, et al. Nephrogenic systemic fibrosis associated with gadolinium use. J Formos Med Assoc. 2008;107(3):270–4.
Cowper SE, et al. Clinical and histological findings in nephrogenic systemic fibrosis. Eur J Radiol. 2008;66:191–9.
Fishman EK, et al. Pseudomembranous colitis: CT evaluation of 26 cases. Radiology. 1991;180:57–60.
Foss C, et al. Gadolinium-associated nephrogenic systemic fibrosis in a 9-year-old boy. Pediatr Dermatol. 2009;26(5):579–82.
Glover SJ, et al. Ophthalmic findings in fetal anticonvulsant syndrome. Ophthalmology. 2002;209:942–7.
Horton KM, et al. CT evaluation of the colon: inflammatory diseases. Radiographics. 2000;20:399–418.
Leiner T, et al. Nephrogenic systemic fibrosis is not exclusively associated with gadodiamide. Eur Radiol. 2007;17:1921–3.
Lexa FJ. Drug-induced disorders of the central nervous system. Semin Roentgenol. 1995;30(1):7–17.
Neustadter LM, et al. Medication-induced changes of bones. Semin Roentgenol. 1995a;30(1):88–95.
Pace MT, et al. Cyclosporin A toxicity: MRI appearance of the brain. Pediatr Radiol. 1995;25:180–3.
Rothenberg AB, et al. Hypervitaminosis A-induced premature closure of epiphyses (physeal obliteration) in humans and calves (hyena disease): a historical review of the human and veterinary literature. Pediatr Radiol. 2007;37:1264–7.
Sharma P, et al. Toxic and acquired metabolic encephalopathies: MRI appearance. AJR Am J Roentgenol. 2009;193:879–86.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree