Ocular Melanoma
 BACKGROUND
BACKGROUND
How does intraocular melanoma rank in terms of incidence among the various eye malignancies?
Intraocular melanoma is #1 among primary cancers (#1 overall is ocular mets).
What is the incidence of ocular melanoma in the U.S.? Is there a race predilection?
4 in 1 million (∼1,500–2,000 cases/yr of ocular melanoma)
Yes. 98% of pts are white.
What are some of the risk factors for developing ocular melanoma?
UV exposure, fair skin, family Hx of ocular melanoma, and personal Hx of cutaneous melanoma
What is the most common site in the eye where ocular melanomas arise?
Uvea, mostly choroidal (85%) > adnexa (10%) > conjunctiva (5%)
What is the cell of origin for ocular melanoma?
Ocular melanoma arises from melanocytes of the uveal stroma (neural crest origin).
What are the components of the uveal tract?
The choroid, ciliary body, and iris comprise the uveal tract.
Name the layers of the choroid from outer to inner.
Layers of the choroid (outer to inner):
1. Haller layer
2. Sattler layer
3. Choriocapillaris
4. Bruch membrane
What are the basic layers of the globe?
Outer fibrous layer (sclera), middle vascular layer (choroid), and inner nerve layer (retina)
What region in the retina is particularly important for color vision?
The macula is important for color vision.
Where is the optic disc relative to the macula?
The optic disc is 2 mm medial to the macula (∼1.5 mm in diameter).
What are the histologic subtypes of ocular melanoma, and which carry the best and worst prognosis?
Spindle cell (best), epithelioid (worst), and mixed (if <50% epithelioid histology)
What % of pts with ocular melanoma present with DM at Dx? What is the most common location?
1%–2% present with DM. The liver is the most common site (5%–20% DM rate over 5 yrs).
What are the different ways melanoma can spread within the globe?
Melanoma can spread intraocularly (through the vitreous, aqueous, or along ciliary vessels/nerves); extraocularly (through the optic nerve, transsclerally, vascular tracking), and through extrascleral extension (10%–15%)
What tumor characteristics predict for DM in ocular melanoma? What is the 5-yr mortality rate in these pts?
Epithelioid histology, large tumors, ant location (ciliary body invasion), monosomy 3, scleral penetration, ↑ mitotic rate, ↑ Ki-67, pleomorphic nucleoli, optic nerve invasion, ↑ MIB-1 index, vascular networks of closed vascular loops, extraocular extension
The 5-yr mortality rate is 55%.
What is the long-term (>10-yr) DM rate from ocular melanoma?
50% of ocular melanoma pts develop DMs at 15 yrs.
 WORKUP/STAGING
WORKUP/STAGING
How do pts with ocular melanoma normally present?
Most (one-third) pts are asymptomatic. Ocular melanoma is usually found on routine exam; otherwise, pts detect it themselves due to vision loss, scotoma, flashing lights, or pain (rare).
What is the workup for a pt with suspected ocular melanoma?
H&P, CBC (LFTs), ophthalmic/funduscopic/slit lamp exam, visual acuity/visual field testing, US (Kretz A-scan, immersion B-scan), fluorescein angiography, MRI, PET/CT to r/o mets
Is Bx commonly done for ocular melanoma?
No. It is a clinical Dx made by exam and imaging. Historically, there is concern that Bx may cause tumor seeding. More recently, Bx is more common for risk stratification/mutational analysis.
What is the genetic alteration most associated with poor prognosis?
BAP1 inactivation. Mutation of 1 allele results in loss of an entire copy of chromosome 3. This correlates with metastatic spread.
What are simulation lesions?
Simulation lesions are lesions that may look like melanoma, such as nevi, hemangiomas, retinal detachment, age-related disciform lesions, and mets.
What feature does ocular melanoma manifest on standard A-scan US?
An acoustic “quiet” zone (central hypoechoic area) vs. mets or hemangiomas (have higher internal reflectivity)
What features do ocular melanomas exhibit on fluorescein angiography?
On fluorescein angiography, ocular melanomas exhibit a double circulation pattern and fluorescein leakage (appearing as hot spots).
What is the T staging of choroidal/ciliary body melanoma based on the latest AJCC (7th edition, 2011) staging guidelines?
AJCC staging is based on 4 tumor size categories that depend on tumor diameter and height as follows (Fig. 24.1):
T1: tumor size category 1
T2: tumor size category 2
T3: tumor size category 3
T4: tumor size category 4
For the T staging of choroidal/ciliary body melanomas, what do the designations a–e represent?
a: no ciliary body involvement/extraocular extension
b: +ciliary body involvement
c: no ciliary body/+extraocular extension ≤5 mm
d: +ciliary body/+extraocular extension ≤5 mm
e: +extraocular extension >5 mm
Describe the AJCC staging for choroidal/ciliary body melanomas.
Stage I: T1aN0M0
Stage IIA: T1b-dN0M0 or T2aN0M0
Stage IIB: T2bN0M0 or T3aN0M0
Stage IIIA: T2c-d, T3b-c, T4aN0M0
Stage IIIB: T3d, T4b-cN0M0
Stage IIIC: T4d-eN0M0
Stage IV: any TN1M0, any T, any NM1
For the M staging of choroidal/ciliary body melanomas, what do the designations a–c represent?
Ma: largest diameter of met ≤3 cm
Mb: largest diameter of met 3.1–8 cm
Mc: largest diameter of met >8 cm
In the Collaborative Ocular Melanoma Study (COMS) staging system, what are COMS small, medium, and large lesions?
COMS staging is based on apical height (AH) and basal diameter (BD):
Small: AH <34 mm, BD up to16 mm
Medium: AH 35–38 mm, BD up to16 mm
Large: AH >8 mm, BD ≥16 mm when AH >2 mm
What are the 10-yr OS rates of COMS small, medium, and large tumors? Pts with DM?
10-yr OS for COMS tumors:
Small: 80%
Medium: 60%
Large: 30%–40%
DM pts: <7 mos
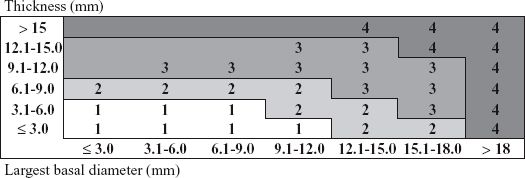
FIGURE 24.1 Primary ciliary body and choroidal melanomas are classified according to the 4 tumor size categories shown. (Edge SD, Byrd DR, Compton CC, et al., eds. AJCC cancer staging manual. 7th ed. New York: Springer; 2010.)
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


