Fig. 1
Screenshot of in-house developed database to register incidental findings on brain MRI. In the upper row, the participant’s basic characteristics will be filled out (e.g., scan date, date of birth). In the left screen, the scan will be displayed. The fields on the right side can be used to characterize potential incidental finding
6 Frequencies of Incidental Findings on Brain MRI in the Rotterdam Study
The overall prevalence of incidental findings on brain MRI examinations in the Rotterdam Study currently is 9.5 % (549 findings in 5800 participants; mean age 64.9 years; Bos et al. 2016). Of these, the most common are meningiomas and cerebral aneurysms (Figs. 2, 3, and 4). Examples of less frequent findings are pituitary abnormalities (i.e., cysts or macroadenomas), arachnoid cysts, or cavernous angiomas. Also, some rare findings such as vestibular or trigeminal schwannomas were found (<1.0 %, included in “Other” in Fig. 2; see also Vernooij et al. 2007).



Fig. 2
Pie chart on the frequency of incidental findings on brain MRI in the Rotterdam Study. The section “Other” includes vestibular schwannoma, arteriovenous malformation, dural fistula, possible glioma, trigeminal schwannoma, orbital dermoid cyst, fibrous dysplasia, intracranial lipoma, atypical cerebellar lesion, ganglioglioma, subependymoma, metastasis, pineocytoma, pharyngeal mucosal asymmetry, colloid cyst of the third ventricle, and expansive lesion in the maxillary sinus
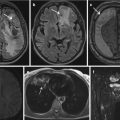
Fig. 3
Example of incidentally discovered aneurysm. T2w MR research scan (left) acquired in a 57-year-old female Rotterdam Study participant shows an aneurysm of the left intracranial internal carotid artery. After hospital referral for further workup, CT angiography (right) confirmed a 9 mm carotid tip aneurysm. The aneurysm was coiled successfully
Fig. 4
Example of incidentally discovered meningioma. FLAIR scan (left panel) of this 68-year-old male Rotterdam Study participant shows a hyperintense broad-based dural mass, compatible with a meningioma. After hospital referral, the presence of a meningioma was confirmed on T1w-Gd scan (right panel). Clinical follow-up was conducted by yearly MRI for 5 years, during which the meningioma did not change and patient was discharged from further follow-up. In a later version of the Rotterdam Study incidental findings protocol, convexity meningiomas <2 cm in size were no longer referred
Interestingly, the prevalence of incidental findings in our population is somewhat higher than reported in other studies (Morris et al. 2009). An important topic to consider with respect to the detection – and thus the frequency – of incidental findings on brain MRI is that this is directly related to multiple nontechnical and technical issues. One of the most important nontechnical issues is the composition of the study population. Important differences in frequency estimates, especially with regard to meningiomas and aneurysms, may arise simply because of the age distribution of the population. In particular for aneurysms, it is well established that these are not present at birth, but develop during aging (Wiebers et al. 2003). Other reasons for differences in frequency estimates across different studies may be due to more technical aspects of the imaging procedure. Examples include the use of specific image sequences, the use of contrast material, and the type of post-processing of the images (van der Lugt 2009). Importantly, in the Rotterdam Study, an optimized MRI protocol is used, and incidental findings are registered by experienced readers with additional review of all recorded incidental findings by a neuroradiologist. Also, the use of a high-resolution proton density-weighted sequence allows a good visualization of the circle of Willis compared to conventional T1-weighted and T2-weighted sequences (Vernooij et al. 2007) and improves the detection of aneurysms. Taken together, these factors may all contribute to differences in the prevalence of specific imaging findings.
Related posts:
 Findings – Ethical Aspects
of Incidental Findings on Multimodal Imaging in UK Biobank
Findings and Their Handling in the Swedish CArdioPulmonary bioImage Study (SCAPIS)
Findings – Ethical Aspects
of Incidental Findings on Multimodal Imaging in UK Biobank
Findings and Their Handling in the Swedish CArdioPulmonary bioImage Study (SCAPIS)
 of Incidental Findings in the Study of Health in Pomerania
of Incidental Findings in the Study of Health in Pomerania
 Findings in a Population Based Study Using Cardiac CT: Experience from the Multi-Ethnic Study of Atherosclerosis (MESA)
Findings in a Population Based Study Using Cardiac CT: Experience from the Multi-Ethnic Study of Atherosclerosis (MESA)
 of Incidental Findings
of Incidental Findings
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


