Orbital Cellulitis, Epidural Abscess, and Meningitis
Scott S. Abedi
CLINICAL HISTORY
20-year-old male with 6 days of worsening left-sided headaches, left eyelid swelling, and redness. The patient was seen previously at an outpatient urgent care and started on cefdinir and prednisone, but now reports worsening of his symptoms.
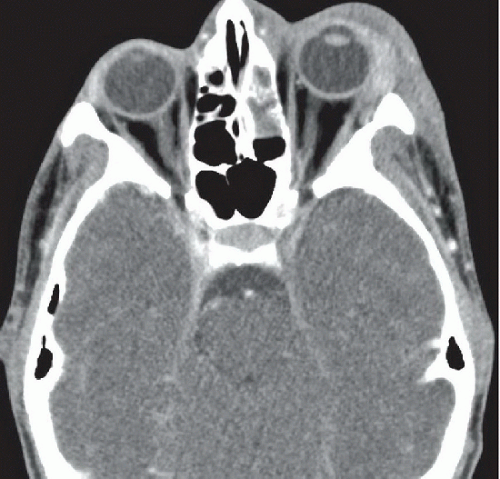 Figure 41A |
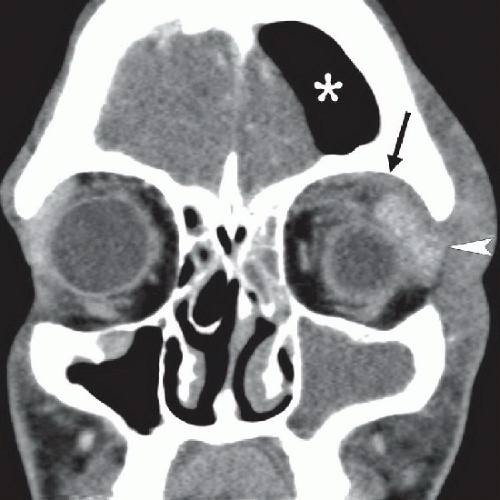 Figure 41B |
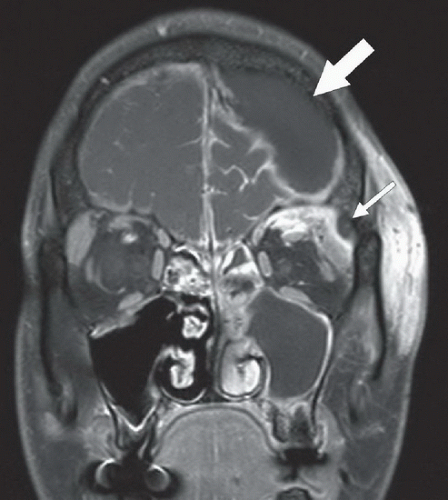 Figure 41C |
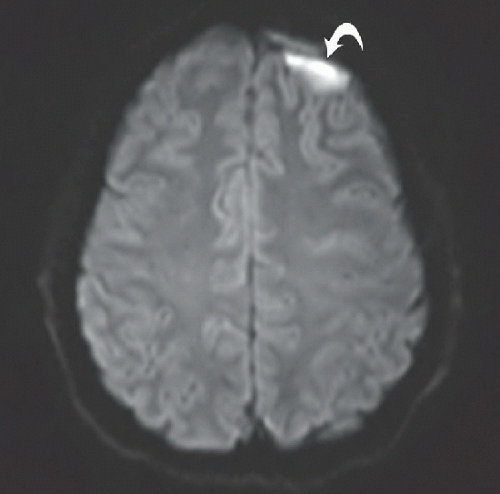 Figure 41D |
FINDINGS
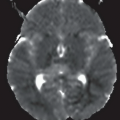
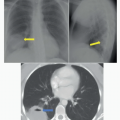
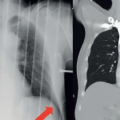
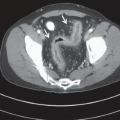
Figure 41A: Axial contrast-enhanced CT at the level of the orbits. There is diffuse left-sided periorbital soft tissue stranding and edema as well as mild left proptosis. The lacrimal gland is prominently enlarged. The left anterior ethmoid air cells are opacified. Figure 41B: Coronal contrast-enhanced CT through the orbits. There is soft tissue stranding (black arrow) of the postseptal fat in the superior orbit that surrounds the superior rectus muscle and enlargement of the left lacrimal gland (white arrowhead). The left maxillary sinus and anterior ethmoid air cells are opacified, whereas there is only a minimal amount of mucosal disease in the right anterior ethmoid air cells and remaining paranasal sinuses. In addition, there is gas (asterisk) within the anterior cranial fossa. Figure 41C: Coronal gadolinium-enhanced fat-suppressed T1WI through the orbits, situated slightly posterior to Figure 41B. There is enhancing soft tissue in the extraconal fat in the superior orbit, displacing the superior rectus downward. There is a small fluid collection in the superolateral quadrant of the orbit abutting the frontal bone (small white arrow). There is an epidural fluid collection (large white arrow) in the anterior cranial fossa with enhancement of the adjacent dura. Note also abnormal thick leptomeningeal enhancement within the sulci of the frontal lobes. Figure 41D: Axial diffusion-weighted image through the brain demonstrates the epidural fluid collection (curved arrow) to have high signal intensity, suggesting restricted diffusion.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


