NONVASCULAR RENAL INTERVENTION Amitha Vikrama Nonvascular renal interventions have come a long way and have significantly reduced the surgical mortality and morbidity. It also paves way for short hospital stay and thus reducing the chances of nosocomial infection. They are usually pinhole or keyhole procedures with less distortion of the anatomy and physiology. They vary from image-guided aspiration/biopsy to percutaneous nephrostomy to complex procedures like ureteric stenting, strictureplasty, percutaneous nephrolithotomy etc. Iversen and Brun were the first to perform percutaneous renal biopsy of native kidneys in 1951. Over the years, newer imaging and biopsy techniques have evolved which have increased the biopsy yield to >95% and significantly reduced the complications of renal biopsy, resulting in decreased mortality rates from 0.12% to 0.02% during the last 50 years NOTE: Solitary renal mass lesions suspicious for malignancy should not be subjected to percutaneous biopsy, as there are chances of tumour seeding along the biopsy track. Excision biopsy is preferred for those lesions as it can be curative. USG-guided renal biopsy is the preferred method over blind biopsies. It avoids nontarget biopsies and reduces bleeding risks. Usually the lower pole of the kidneys is preferred site in native renal biopsy. The needle has to be directed into the lower cortex and care taken to avoid renal medulla and collecting system. 18G trucut biopsy needles are usually used in adults. In paediatric population, 20G can be used. Rarely, Coaxial technique is used in very obese patients and in those who are unable to lie prone. It is usually done as an inpatient procedure. Four hours of fasting is required to prevent aspiration of gastric contents during the procedure. Antiplatelets and anticoagulants are stopped at least 3–5 days prior. Informed written consent has to be taken after explaining the risks and benefits of the procedure. Patient is to be positioned in prone and USG-guided marking of the site of biopsy done prior to cleaning and draping. The depth of the renal cortex from the skin surface has to be noted. If the ribs are coming in line with the lower pole cortex, then a cranially angulated path is preferred. After infiltration of 2% lignocaine, the biopsy needle is advanced up to and not into the lower pole cortex. As the kidney keeps moving with respiration, the biopsy should be properly timed to avoid hitting the collecting system and medulla. This method is real-time ultrasound guided renal biopsy (Fig. 10.21.1.1). There is another method practiced in few of the institutes where the location of lower pole of the kidney is marked on the skin after ultrasound screening. The marking corresponds to the lower most renal cortex at the end of normal inspiration and the biopsy path will be perpendicular to the bed without any craniocaudal or mediolateral angulation. The distance between the skin and the renal cortex is measured. The patient will be instructed strictly not to change his position. Then the biopsy will be done blindly without any real time USG guidance. With this method, more number of patients can be biopsied in a short interval time. In a transplanted kidney, which is usually grafted in the iliac fossa, biopsy can be obtained from upper or lower pole. Points to remember: Cortical tangential and cortical non tangential approaches have been described (Fig. 10.21.1.2). Cortical tangential approach is described to have better diagnostic yield with lesser complications. In this approach, the needle track will be almost parallel to the capsule so that only the cortical tissue is targeted (Fig. 10.21.1.3A–C). Renal biopsy can also be done with coaxial technique. In this method, a coaxial needle, one size bigger than the biopsy needle, usually 17G, is inserted up to the renal capsule. The stylet is then removed and the 18G biopsy needle is inserted through the coaxial needle and the required number of biopsy specimens obtained. After this, the rent in the capsule can be sealed off with gelatine plugs before removing the coaxial needle. This helps in preventing bleeding complications. In patients with high risk of bleeding due to coagulation abnormalities, transjugular renal biopsy can be done in which renal vein is cannulated and biopsy done from within (Fig. 10.21.1.3D–F). In obese patients who cannot lie prone, biopsies are done in lateral or oblique lateral positions under CT or USG guidance. CT guidance is especially helpful when the visualization of the kidney is difficult on ultrasound. In these cases, coaxial technique is always helpful. In 2019, KHA-CARI guidelines were first published for renal biopsy. A few of the salient recommendations are given below: It is an image-guided procedure in which the renal pelvicalyceal system is accessed percutaneously which is predominantly used for decompressing an obstructed system and also for various other therapeutic procedures. It is usually done under local anaesthesia and IV sedation. Major procedures might require general anaesthesia. All routine preprocedural blood tests and coagulation profile should be done. Appropriate antibiotics are administered intravenously prior to the procedure. 21G needle, 018 and 035 wires, appropriate dilators, sheath and pigtail drainage catheter. Ultrasound and fluoroscopy is required for guidance. Patient is usually positioned prone on the table. Under special circumstances, lateral or oblique positions are also used. After instillation of local anaesthesia, a 21G needle is used to access the renal calyx under USG guidance. Once the urine flow is seen, nonionic contrast is injected to delineate the renal collecting system. A 018 wire is passed through the needle into the pelvicalyceal system and later exchanged for a 035 wire. Appropriate tissue dilators are used to dilate the track before placing a pigtail drainage catheter. The drain is secured by stay sutures and connected to a urobag. The initial urine sample is to be sent for culture and sensitivity (Figs. 10.21.1.4–10.21.1.6). Ureteric stenting was first described by Zimskind et al endotracheal tube al in 1967. It is one of the commonest procedure done in urology practice It is usually done after doing a percutaneous nephrostomy. The percutaneous nephrostomy (PCN) drain is replaced with a 6F or 8F sheath over a guidewire and ureterogram is obtained to assess the site of stricture or obstruction. Using a catheter and guide wire combination, the stricture is negotiated and the exchange length hydrophilic wire is parked in the bladder. The ureteric length is measured and appropriate-sized double J (DJ) stent is inserted over the wire. Care is taken to get the loops formed at both ends of the DJ stent so that stent migration is prevented (Fig. 10.21.1.7). A variety of delivery systems are available for the deployment of the ureteric stent exist: pusher mechanism, string release and sheath (similar to an inferior vena cava (IVC) filter). Post stent insertion, the nephrostomy drain can be retained for a couple of days. The drain is closed externally and USG screening is done the next day to confirm antegrade flow after which the drain can be removed.
10.21: Other renal vascular interventions
Introduction
Renal biopsy
Indications
Contraindications
Relative contraindications
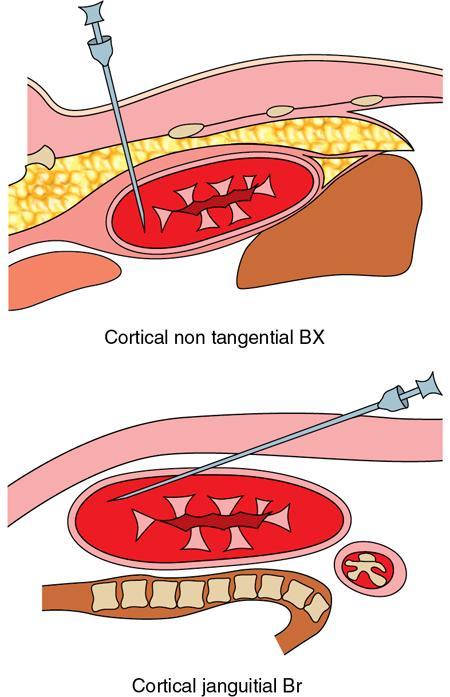
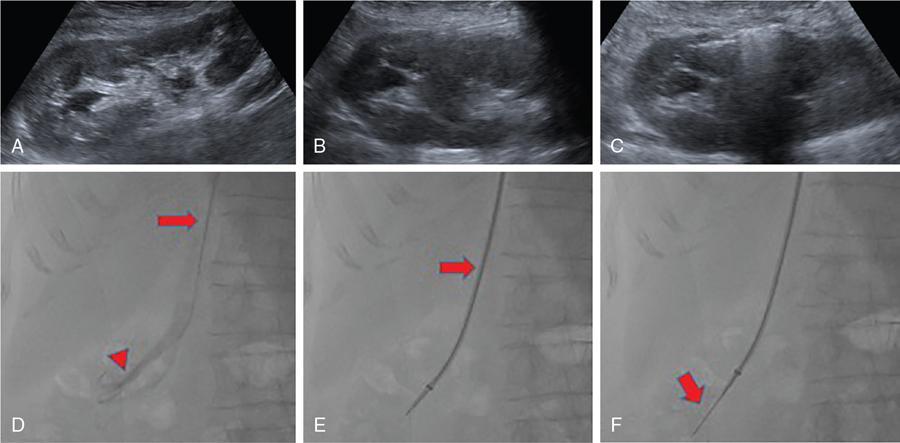
Techniques

Biopsy of renal transplants
Guidelines
Percutaneous nephrostomy
Indications
Contraindications
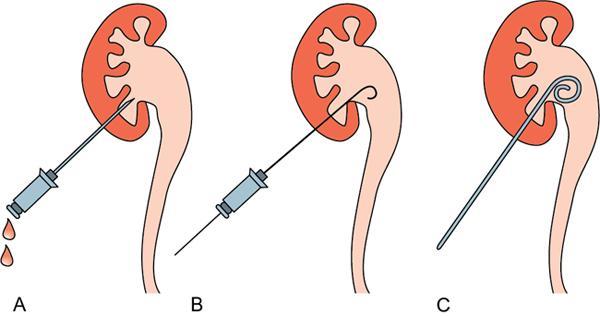
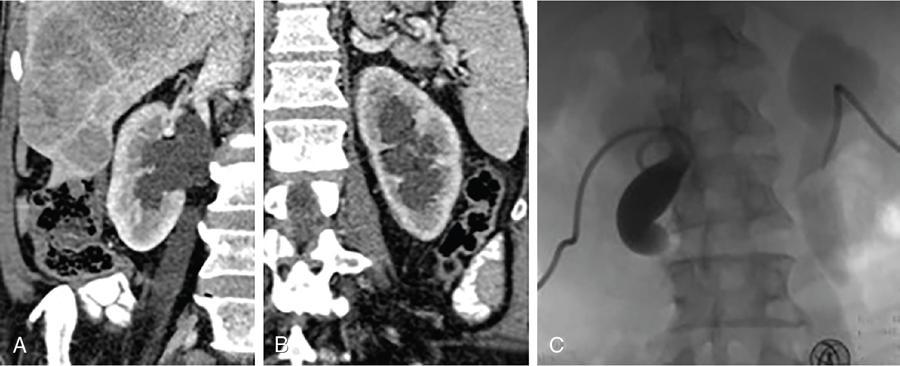
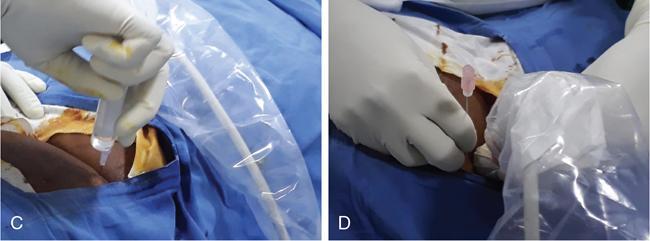
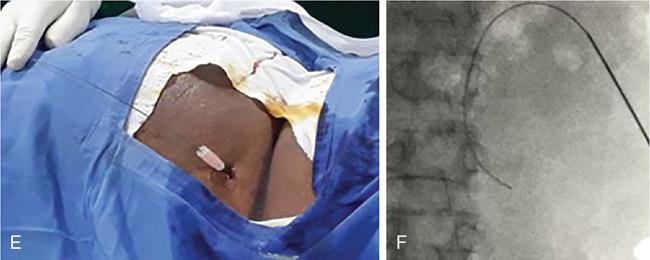
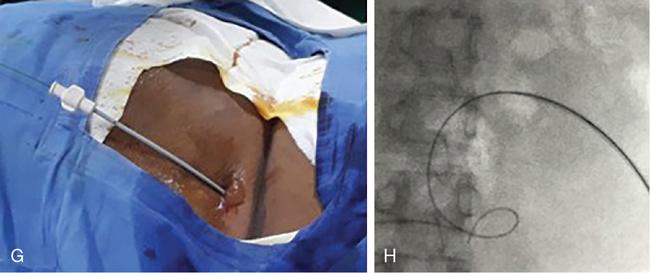
Technical aspects
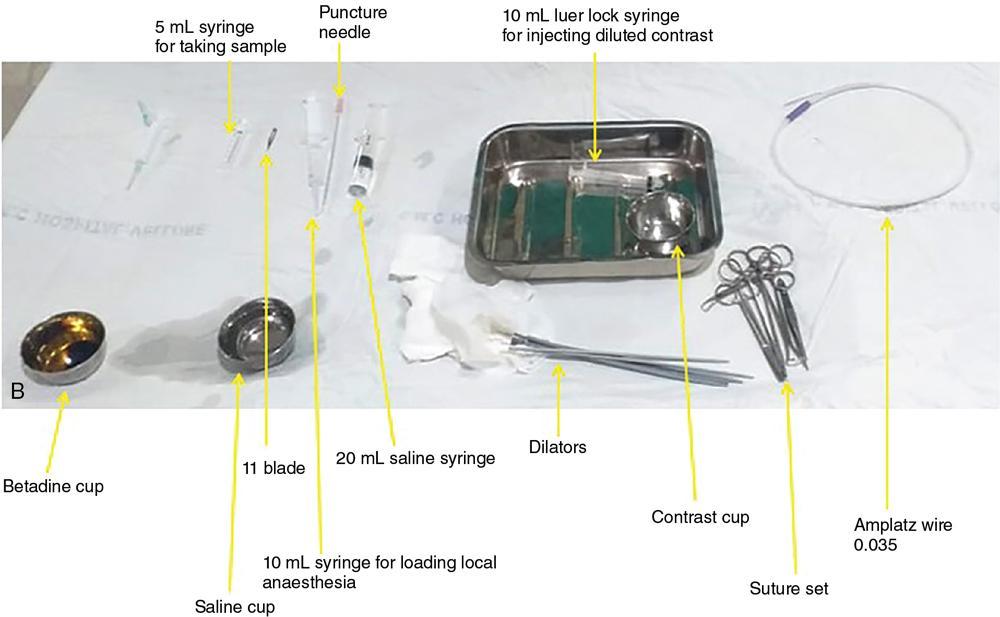
Materials

Complications
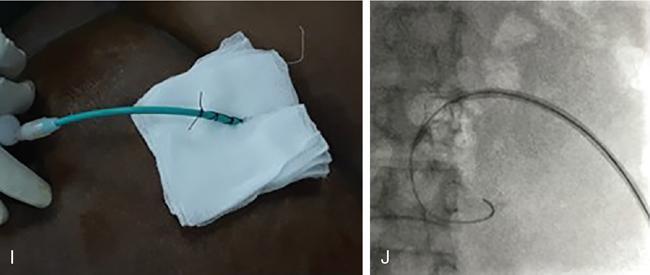
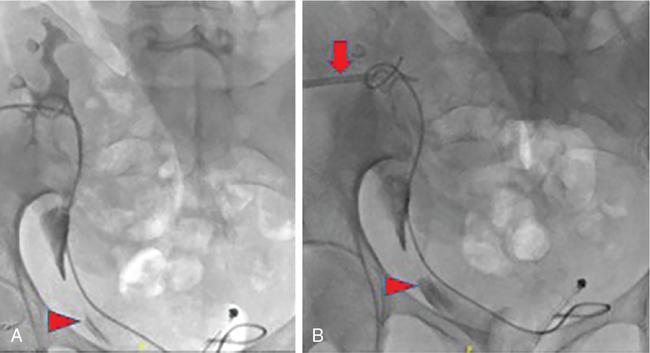
Percutaneous antegrade ureteric DJ stenting
Indications
Contraindications
Technique
Tips for complex cases
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


