Ovarian torsion is an acute gynaecological condition characterized by partial or complete rotation of the ovary on its pedicle within its ligamentous support, resulting in vascular compromise with obstruction to venous and lymphatic outflow and arterial inflow. Even though the term ‘ovarian torsion’ is routinely used, a more appropriate terminology would be ‘adnexal torsion’, as the fallopian tubes are very often torsed along with the ovaries, in up to 67% of the cases. Adnexal torsion refers to involvement of the ovaries, fallopian tubes or both and can present in females of all age groups. Early and accurate diagnosis with surgical intervention is imperative to reduce morbidity and prevent complications like ovarian and tubal necrosis with loss of function, peritonitis and sepsis. This is especially important in children and young women to maintain normal ovarian function and preserve fertility.
Rarely, other forms of torsion including isolated torsion of the fallopian tube and torsion of paraovarian, paratubal and broad ligament cysts may be seen.
The clinical presentation of ovarian torsion is frequently nonspecific and can mimic other abdominopelvic emergencies. Hence, imaging plays a major role in prompt diagnosis with appropriate surgical management.
Epidemiology
Torsion is the fifth most common gynaecological emergency accounting for 2.7% of cases. A retrospective study found that 14.8% of cases of adnexal masses treated surgically were due to torsion.
Torsion can occur at any age but is most prevalent in women of the reproductive age group, with 17%–20% age of patients presenting in pregnancy, more so before 20 weeks’ gestational age. It may also be seen in the paediatric age group (most commonly in early adolescence, immediate postmenarchal period and in the first year of life) and in postmenopausal patients. Torsion has also been described in the foetal period.
Pathogenesis
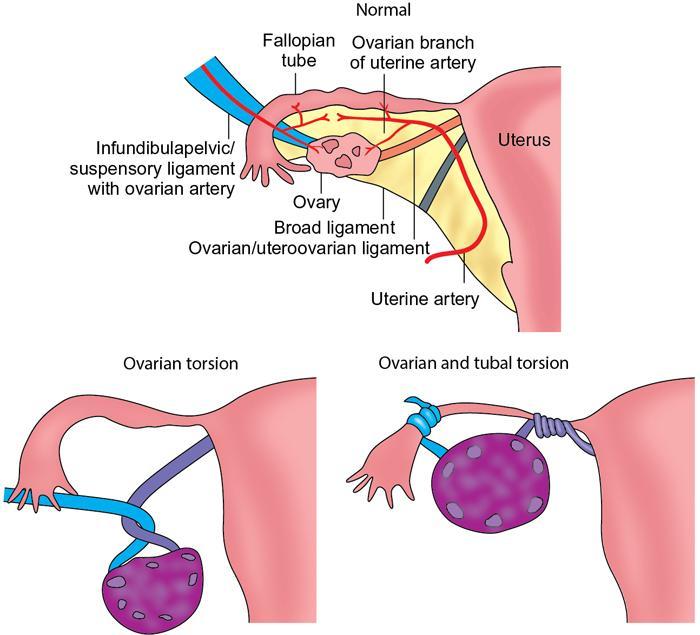
The torsed ovary twists along the axis of the suspensory/infundibulopelvic ligament (which attaches the ovary to the pelvic sidewall and contains the ovarian vessels) and the utero-ovarian ligament (which attaches the medial aspect of the ovary to the side of the uterus and contains the uterine vessels including its ovarian branches). As the adnexal tissue is not fixed, a mass lesion or a large cyst can serve as a lead point or fulcrum and induce torsion. Initially, the low pressure thin-walled venous and lymphatic system is obstructed. The arteries are less susceptible at the outset owing to their muscular walls. Continued arterial perfusion with obstructed venous and lymphatic outflow results in significant ovarian enlargement with stromal oedema, and further vascular compromise. Ultimately, persistent torsion results in arterial thrombosis with ischaemia leading to haemorrhagic infarction and ovarian necrosis. In case the fallopian tubes are involved, tubal necrosis can result (Fig. 11.16.1.1).
Massive ovarian oedema is a rare condition described with intermittent partial torsion. It is due to venous and lymphatic obstruction with preserved arterial supply, resulting in persistently raised capillary hydrostatic pressure and grossly enlarged and oedematous ovary, which may mimic a tumour.
Risk factors
• Torsion predominantly occurs in ovaries >5 cm in size, with mass lesions or cysts (functional and pathological), but may sometimes be seen with normal ovaries.
• As many of the ovarian masses or cysts are seen in the reproductive period and are related to reproductive hormones, torsion is more often seen in this age group, pregnancy and in patients undergoing treatment for infertility with ovulation induction in whom large follicular cysts and ovarian hyperstimulation syndrome can develop. In adults, tumours and cysts serve as the lead point for torsion in a large number of patients. Paraovarian cysts can also predispose to torsion.
• Some of the common lead points seen are follicular cysts, haemorrhagic cysts, corpus luteal cysts and tumours like mature cystic teratomas, cystadenomas, fibromas and Brenner cell tumours.
• The most common associated tumour is the mature cystic teratoma.
• The presence of ovarian masses also predisposes to torsion in foetuses, neonates and premenarchal patients.
• Torsion in normal ovaries is seen more often in adolescents. Normal ovaries were demonstrated in more than half of the patients with torsion presenting at less than 15 years of age.
• Occasionally, recurrent torsion can occur. Recurrence was seen in about 11% of patients in one studied series. Recurrence can occur on the same side or asynchronously on the contralateral side (Table 11.16.1.1).
Elongated or mobile fallopian tubes and mesosalpinx
Functional cysts like follicular cysts, haemorrhagic cysts, polycystic ovaries and corpus luteal cysts
Elongated utero-ovarian ligament
Following ovulation induction in patients with infertility, resulting in enlarged cystic ovaries and ovarian hyperstimulation syndrome
Fallopian tube spasm
Benign neoplasms like mature cystic teratoma (most common tumour), cystadenoma, fibroma and Brenner cell tumour
Vigorous exercise
Abrupt increase in intra-abdominal pressure
Torsion rare in endometriosis and pelvic inflammatory disease due to adhesions.
Unusual in malignancies due to peritumoural invasion and fibrosis, leading to immobility.
More common on the right side due to lack of protective effect of sigmoid colon, and longer right-sided utero-ovarian ligament.
Clinical features
The typical presentation is the sudden onset of lower abdominal or pelvic pain, often associated with nausea and vomiting. Low-grade fever is occasionally present.
However, these symptoms are nonspecific and may be seen in other conditions like ectopic pregnancy, ruptured ovarian cyst, tubo-ovarian abscess, endometriosis, degenerating leiomyomas, ureteric colic, appendicitis and diverticulitis. Sometimes, the presentation can be intermittent and prolonged due to multiple episodes of torsion and detorsion, manifesting as alternating episodes of acute pain followed by asymptomatic periods.
Physical examination may reveal localised or diffuse tenderness and a palpable pelvic or lower abdominal mass. Peritoneal signs may be seen in untreated and persistent torsion due to adnexal necrosis and peritonitis.
Laboratory investigations
These should include:
• Serum chorionic gonadotropin hormone: To confirm or exclude pregnancy as torsion is fairly common in pregnancy. Also, to exclude ectopic pregnancy which is a common differential diagnosis in such patients.
• White blood cell count: Moderate leukocytosis may be seen.
• Haematocrit: May suggest haemorrhagic necrosis.
• Serum tumour markers: If indicated.
• A link has been reported between raised serum interleukin 6 (IL-6) and torsion.
Diagnostic imaging
The imaging appearances vary with:
• The duration and degree of torsion.
• Whether imaging is performed in the initial stages of congestion and oedema, or in the later stages of haemorrhagic infarction.
• Presence if any of a mass lesion or cyst.
Grey-scale ultrasound with doppler examination
This is the first-line imaging modality. Studies have shown sensitivities for the diagnosis of torsion on ultrasound ranging from 42% to 75%. Another study assessing the effectiveness of ultrasound in ovarian torsion demonstrated a positive predictive value of 87.5% with specificity as high as 93.3%. Ideally, a transabdominal scan followed by a transvaginal scan when feasible should be performed.
Computed tomography
A computed tomography (CT) study is generally performed in the setting of a female patient presenting with lower abdominal or pelvic pain, and the differential diagnosis includes bowel and urological causes like appendicitis, diverticulitis, renal or ureteric colic, in addition to gynaecological causes.
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is especially useful when the initial ultrasound or CT examination is ambiguous or reveals an indeterminate adnexal lesion in a female patient presenting with acute pelvic pain. MRI depicts the adnexal abnormality better than CT. The MR sequences required are T1-weighted image (T1WI), fat sat T1WI, T2-weighted image (T2WI), diffusion-weighted imaging (DWI) and gradient echo/susceptibility-weighted imaging (GRE/SWI). In restless and pregnant patients, ultrafast T2-weighted MR sequences like single-shot fast spin echo (SS-FSE)/half-fourier acquisition single-shot turbo spin echo imaging (HASTE) and fast imaging employing steady-state acquisition (FIESTA)/true fast imaging with steady-state free precession (TRUFI) can be performed. Contrast MRI may be performed to assess adnexal viability and necrosis, to identify the swirling appearance of the twisted pedicle and for evaluation of an underlying mass lesion.
Imaging findings common to ultrasound, CT and MR
• There is a wide spectrum of appearances of the torsed lesion ranging from heterogeneous to either predominantly solid or cystic.
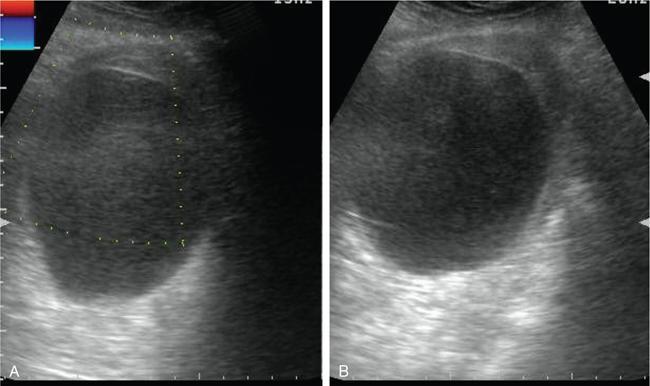
• The most common and consistent finding is an enlarged ovary which is due to oedema with vascular and lymphatic engorgement. Ovarian enlargement is seen even in the absence of an associated mass lesion. In addition to enlargement, the affected ovary can show a more rounded appearance. Rarely, normal-sized ovaries have been described in a minority of cases.
• The follicles/cysts are seen at the periphery with a ‘string of pearls’ appearance, and central afollicular stroma, due to stromal oedema and/or haemorrhage.
• The most important and definitive finding which confirms the diagnosis of torsion is the demonstration of the twisted vascular pedicle with a ‘whirlpool sign’ (clockwise or counter-clockwise swirling of vessels around a central axis). The twisted pedicle can include the thickened fallopian tube (>10 mm).
• Cyst wall thickening is sometimes present.
• The torsed ovaries may be abnormally placed, in the midline or paramidline location, superior to the uterine fundus or on the contralateral side. The torsed adnexa may be located far anteriorly or posteriorly in the pouch of Douglas.
• Adjacent free fluid (ascites or haemoperitoneum) may be present.
Specific grey-scale ultrasound imaging features
• The ovarian stroma can appear hypoechoic in the stage of congestion and oedema, and heterogeneous or hyperechoic in the stage of haemorrhagic infarction.
• Other appearances of the twisted pedicle with/without the fallopian tube include a target or beaked appearance (echogenic mass with multiple concentric hypoechoic stripes), snail-shell appearance, an enlarged hypoechoic or echogenic mass or an ellipsoid or tubular mass with heterogeneous internal echoes.
• Some cysts show echogenic material within due to haemorrhage associated with ischaemia and infarction.
• Abnormal location of a torsed ovarian cyst in the midline location can result in the ‘double bladder’ sign.
• Tenderness of the torsed adnexa can be elicited only on ultrasound as an imaging modality.
• In massive ovarian oedema, a grossly enlarged ovary is seen with severe stromal oedema and peripherally displaced follicles. This can mimic a solid tumour and can occur in torsion of normal ovaries as well as in torsed ovaries with benign neoplasms. Ultrasound and MRI are more useful in diagnosing this condition.
Colour doppler
The findings depend upon the severity and duration of torsion and, therefore, range from complete absence of flow to normal flow. It is crucial to obtain correct Doppler settings which can be done on the contralateral side, before assessing the affected side.
• Though the classical finding described is the lack of arterial flow, the most common abnormality seen is reduced or absent venous flow. The veins are initially affected due to their thin compliant walls.
• Lack of arterial flow is typically associated with venous flow abnormality.
• The ‘whirlpool sign’ on Doppler imaging is seen as circular or coiled vessels within the twisted pedicle.
• Presence of flow within the vascular pedicle indicates ovarian viability.
• Lack of reversal of diastolic flow is noted in some patients.
• The absence of central venous flow within the ovary is said to represent nonviability.
• However, it is exceedingly important to remember that a normal Doppler study does not exclude torsion. This may be due to intermittent episodes of torsion, with the Doppler study performed during a phase of detorsion. Another reason could be dual arterial supply to the ovaries (ovarian artery from the aorta and ovarian branches from the uterine artery).
Specific CT and MRI features
• Multiplanar reformation is very often required to demonstrate the specific finding of the twisted pedicle ‘whirlpool sign’. Contrast-enhanced CT better delineates this in comparison to unenhanced CT. On MRI, it is best seen on T2WI.
• The sagittal plane is especially useful in identifying thickened tubes, which can appear as a tubular protrusion extending from the superiorly located adnexal mass towards the uterus located inferiorly. This occurs because the lower pelvis is too small to accommodate the torsed adnexal mass.
• In addition to the ‘whirlpool sign’ which is not always seen, other appearances of the twisted pedicle/thickened tubes include a tubular lesion, solid amorphous lesion, target appearance or a beaked or serpentine-like protrusion extending from the uterus and partially covering the adnexa.
• In the initial nonhaemorrhagic state of oedema and congestion, the thickened tube/pedicle/ovary appears hypodense on CT/hypointense on T1WI and hyperintense on T2WI.
• In the later stages of haemorrhagic infarction and necrosis, unenhanced CT reveals haemorrhage (>50 HU) presenting as an intraovarian haematoma or layering haematocrit level, haematosalpinx or haemoperitoneum. On MRI, they appear hyperintense on T1WI and fat suppression T1W1 (FST1WI), hypointense/hyperintense on T2WI and hypointense on GRE/SWI. T2 hypointensities within the adnexa favour nonviability. Although similar findings may be seen in other acute conditions like ectopic pregnancy, endometriosis with rupture or haemorrhagic ovarian cyst, the presence of a twisted pedicle confirms the diagnosis of ovarian torsion. The presence of adnexal haemorrhage in torsion is indicative of nonviable ovaries.
• A peripheral T1 and FST1 hyperintense rim of an ovarian haematoma, representing subacute haemorrhage, indicates haemorrhagic infarction and favours the diagnosis of torsion in the appropriate clinical setting.
• MRI is the best modality to identify ovarian stromal oedema and haemorrhage.
• Concentric or eccentric thickening of a cyst wall (>3 mm) may be present with intracystic heterogeneities due to haemorrhage. Eccentric smooth wall thickening converging on a thickened fallopian tube favours haemorrhagic infarction.
• Engorged vessels due to venous congestion may be present on the ipsilateral side distal to the torsion.
• Ipsilateral deviation of the uterus may be noted due to the adnexal ligament shortening.
• Poor or absent adnexal enhancement implies infarction with necrosis.
• Periadnexal infiltration or obliteration of the adjacent fat planes is due to the acute presentation.
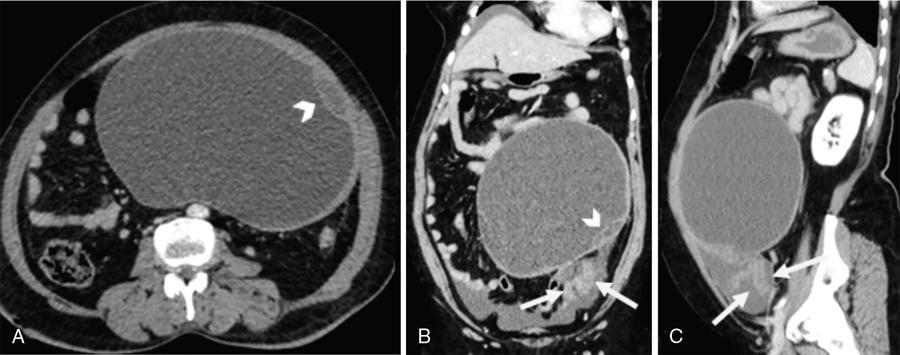
Fig. 11.16.1.2Benign serous cyst with torsion in a 52-year-old postmenopausal lady presenting with acute left-sided abdominal pain. (A) Axial CT section with (B) coronal and (C) sagittal reformations shows a large cyst in the central and left lower abdomen with few septae within (arrowheads). (B and C) An enhancing thickened twisted pedicle is noted extending from the pelvis up to the cyst (arrows). Surgery and histopathology confirmed features of benign serous cyst with torsion.
Fig. 11.16.1.3Adnexal torsion without mass lesion: (A) Axial and (B) coronal T2W1 in an 18-year-old with intermittent episodes of severe lower abdominal pain shows an enlarged left ovary located in the midline in the pouch of Douglas (arrows). Multiple small follicles are seen displaced to the periphery (arrowheads). (C) There is extensive haemorrhage within the ovarian stroma as confirmed with blooming on GRE (asterisks). (A and B) Note the thickened pedicle including the fallopian tube (curved arrows). Oophorectomy was performed for the gangrenous ovary.
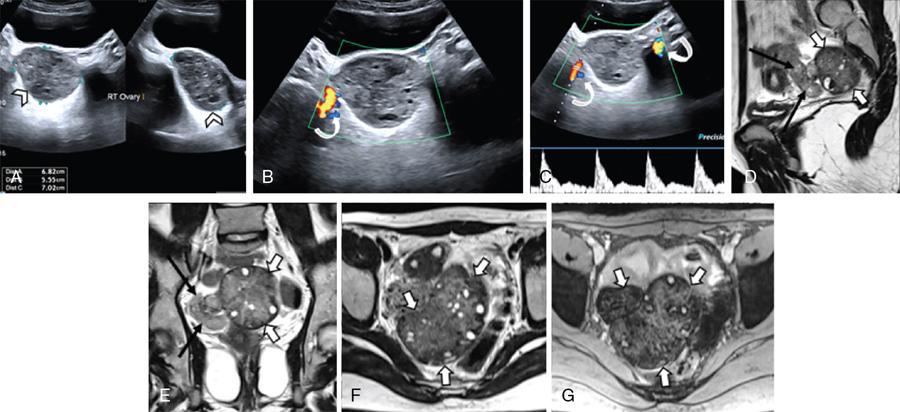
Fig. 11.16.1.4Adnexal torsion without mass lesion: (A) Grey-scale USG in an adolescent girl with symptoms of acute pelvic pain, nausea and vomiting shows an enlarged right ovary (arrowheads) with heterogeneous stoma and multiple small follicle. (B and C) Colour flow imaging shows arterial flow within the pedicle (curved arrows), but absent intraovarian vascularity. (D) Sagittal, (E) coronal, (F) axial T2WI and (G) GRE confirms the enlarged right ovary with haemorrhagic stroma and small follicles, situated within the pouch of Douglas in the midline (short thick arrows). Note the thickened right pedicle including the fallopian tube (long thin black arrows). Detorsion with oophoropexy was performed.
Fig. 11.16.1.5Ovarian hyperstimulation syndrome with right adnexal torsion: A 30-year primigravida with in vitro conception presented at 8 weeks’ gestational age with severe right lower abdominal pain and vomiting. (A, B and D) T2WI displays grossly enlarged right ovary (arrowheads) with multiple cysts. The ovarian stroma is hypointense on (A, B and D) T2WI and (E) GRE due to haemorrhage (asterisk). (C and F) Presence of a twisted pedicle is noted (short thick arrows). (D) A dilated jejunal loop is seen adherent to the right ovary (curved arrow). (B and F) The left ovary is also enlarged, though to a lesser extent, with multiple cysts (long thin white arrows). Emergency laparotomy with right salpingo-oophorectomy with adhesive band release for torsion of gangrenous right ovary, and small intestinal obstruction was done.
Fig. 11.16.1.6Corpus luteal cyst with torsion: (A) Grey-scale USG with (B) Doppler in a 26-year primigravida (conceived following treatment for infertility), complaining of sudden severe right-sided pelvic pain at 8 weeks’ gestational age shows an enlarged right ovary with two cysts (arrowheads). No intraovarian flow is seen. However, arterial flow is present in the pedicle (curved arrow). (D–F) T2WI show the enlarged right ovary with two cysts (short thick arrows), one of which has hypointense walls due to haemorrhage, as confirmed on (C) GRE (thin black arrow). (G) Coronal T2WI depicts the thickened and twisted vascular pedicle with the ‘whirlpool’ appearance (thin white arrows). (H and I) Following laparoscopic detorsion with fluid aspiration from the larger cyst, a repeat USG scan with Doppler 2 weeks later shows reduction in the size of the ovary with a collapsed cyst with heterogeneous echoes (asterisk) and (J) revived normal intraovarian vascularity. The patient subsequently had a normal delivery.
Fig. 11.16.1.7Benign mature cystic teratoma with torsion: A 30-year-old woman presented with episodes of lower abdominal pain and vomiting. (A) USG showed a complex right ovarian cyst (arrowheads) with septae. (B) No intralesional vascularity noted on Doppler examination. (C) Coronal and (D) axial T2WI, (E) axial TIWI and (F) FST1WI showed a complex right ovarian cyst, with an area of signal intensities consistent with fat (asterisk). (C) Thickened and twisted pedicle with the pathognomic ‘whirlpool’ appearance is also noted (thick arrows). Laparoscopic right ovariotomy with excision of the tumour was done.
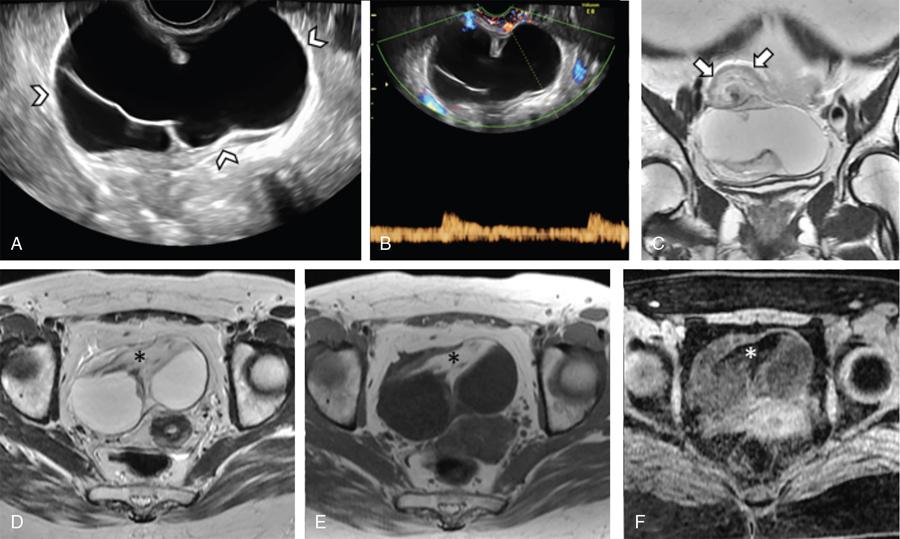
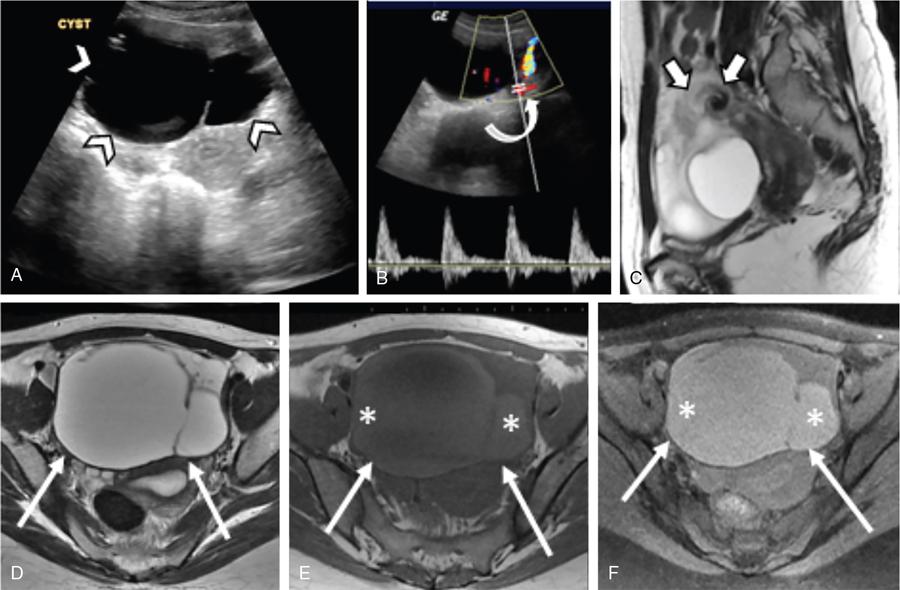
Fig. 11.16.1.8Benign seromucinous cystic tumour with torsion in a 31-year-old woman with complaints of acute lower abdominal pain. (A) Grey-scale ultrasound shows a large cyst with thin septae anterior to the uterus (arrowheads). (B) Colour flow Doppler reveals arterial flow in the pedicle with no flow within the cyst (curved arrow). (C) Sagittal T2WI shows the classical ‘whirlpool’ sign of the twisted pedicle (short thick arrows). (D) Axial T2WI, (E) T1WI and (F) FST1WI demonstrates the midline anterior location of the cyst (thin arrows), with the contents appearing hyperintense on T1WI and FST1WI (asterisks). Emergency laparoscopic cystectomy was done with a final diagnosis of –Benign seromucinous tumour.
Fig. 11.16.1.9Immature teratoma with torsion: A 16-week-pregnant woman complained of sudden onset left-sided abdominal pain. (A) USG with (B) Doppler reveals a complex mixed solid cystic lesion in the central and left side of abdomen (arrowheads), with minimal internal vascularity (thin arrows). (C and D) Coronal FS FIESTA and (E) HASTE shows a thickened, twisted and stretched vascular pedicle (short thick arrows) extending from the gravid uterus vertically up to the tumour (arrowheads). Oophorectomy was done followed by chemotherapy.
Differential Diagnosis in a Female Patient With Acute Pelvic Pain and Adnexal Mass
Adnexal Torsion
Ectopic Pregnancy
Ruptured/Haemorrhagic Ovarian Cyst
Tubo-Ovarian Abscess
Twisted pedicle
Present
Absent
Absent
Absent
Beta-hCG
Negative
Positive
Negative
Negative
Vaginal bleeding
Rare
Common
Rare
Rare
Fever
If present, mild
Absent
Absent
More significant
Presentation
Acute, occasionally intermittent
Acute or chronic
Acute
More indolent course
Peripherally placed follicles in ovarian torsion vs polycystic ovarian syndrome: Unilateral and acutely symptomatic in torsion, bilateral with no acute symptoms in PCOS.
Management
The aim of emergency surgery is to conserve viable ovarian tissue, especially in premenopausal patients, and prevent complications like peritonitis and sepsis. Based on the age group and findings, the surgical options include detorsion and ovarian conservation, cystectomy, oophorectomy or salpingo-oophorectomy. Ovariopexy may be performed to fix the ovaries.
Conclusion
Adnexal torsion is a gynaecological emergency which requires prompt diagnosis and immediate surgical intervention to prevent the loss of ovarian function and other complications such as peritonitis and sepsis. As the clinical presentation is nonspecific, imaging comprising ultrasound with Doppler examination, CT and MRI play a significant role in diagnosing this condition. MRI is commonly used as a problem-solving modality when findings are indeterminate on ultrasound or CT. The ideal imaging protocol would be ultrasound with Doppler, followed by MRI in equivocal cases. Even though an enlarged ovary on the symptomatic side is the most common finding, the pathognomonic feature is a twisted vascular pedicle. In view of a spectrum of imaging findings, the radiologist must maintain a high index of suspicion in diagnosing this condition, especially when an adnexal mass is seen in a female patient presenting with acute lower abdominal or pelvic pain (Box 11.16.1.1) (Table 11.16.1.3).
Definition: Partial or complete rotation of the ovary ± fallopian tube, on its vascular pedicle within its ligamentous support, resulting in vascular compromise with obstruction to arterial inflow and venous and lymphatic outflow.
Terminology:
• ‘Adnexal torsion’ more appropriate rather than ‘ovarian torsion’ as the tubes are often torsed along with the ovaries. Adnexal torsion = ovarian ± tubal torsion
• Most common is combined ovarian and tubal torsion
• Rare forms of torsion are isolated fallopian tube torsion, paraovarian, paratubal or broad ligament cyst torsion
Age:
• At any age from the foetus to postmenopausal
• Most common in the reproductive age group and pregnancy
Pathogenesis: Torsion of the ovaries/adnexa within the supporting ligaments leads to vascular compromise with initial venous and lymphatic obstruction resulting in ovarian enlargement with stromal oedema and congestion, subsequently followed by arterial compromise with haemorrhagic infarction and necrosis of the affected adnexa.
Risk factors:
• Ovaries >5 cm in size, especially with functional or pathological cysts/tumours which serve as lead points
• Functional cysts: Follicular cysts, polycystic ovaries, corpus luteal cysts, enlarged cystic ovaries or ovarian hyperstimulation syndrome following treatment of infertility
• Pathological cysts and tumours: Mature cystic teratomas (most common tumour), cystadenomas, fibromas and Brenner cell tumours
• Torsion in normal ovaries more common in children
• Predisposing factors in normal ovaries are elongated or mobile fallopian tubes and mesosalpinx, elongated utero-ovarian ligament, fallopian tube spasm, vigorous exercise and abrupt increase in intra-abdominal pressure
• Torsion rare in endometriosis, pelvic inflammatory disease and malignant tumours
Clinical features:
• Sudden onset of lower abdominal or pelvic pain, nausea, vomiting, occasional fever
• Palpable pelvic or lower abdominal mass
• Peritoneal signs ±
• Occasional subacute or prolonged history due to multiple intermittent episodes of torsion and detorsion
Management: Surgical. Conservation of ovarian tissue important in paediatric and reproductive age groups.
• Whether imaging is performed in the initial stages of congestion and oedema, or later stages of haemorrhagic infarction and necrosis
• Presence if any, of a mass lesion or cyst
FINDINGS COMMON TO USG, CT
Ipsilateral ovarian enlargement – most common finding
Twisted vascular pedicle (can include the fallopian tube), if present – pathognomonic finding ‘whirlpool sign’
Thickened fallopian tube (considered when >10 mm)
Peripherally placed ovarian follicles with central afollicular stroma
‘String of pearls’ appearance
Presence of coexistent ovarian mass or cyst altering the appearance
Wide spectrum of appearances of the torsed adnexa ranging from heterogeneous/predominantly solid/predominantly cystic
Intraovarian haemorrhage (within stroma, follicles, cyst or mass), haematosalpinx
Concentric or eccentric cyst wall thickening (>3 mm)
Malpositioned adnexa: In the midline, paramidline or contralateral side
Free fluid: Haemoperitoneum or ascites
USG
CT
MRI
• In the initial stages of oedema and congestion, ovarian stroma appears hypoechoic
• In the later stages of haemorrhagic infarction, appears mixed echogenic or hyperechoic
• Internal echoes within a cyst or follicle due to haemorrhage
• In the initial stages of oedema and congestion, appears hypodense
• In the later stages of haemorrhagic infarction: Intraovarian haemorrhage, haematosalpinx and haemoperitoneum (>50 HU on CT)
• In the initial stages of oedema and congestion, appears hypointense on T1WI and hyperintense on T2WI
• In the later stages of haemorrhagic infarction: Intraovarian haemorrhage, haematosalpinx and haemoperitoneum may be seen – hyperintense on T1WI and FST1WI, hyperintense/hypointense on T2WI, hypointense on GRE
Peripheral T1 and FST1 hyperintense rim of an ovarian haematoma
Other appearances of the twisted pedicle with/without fallopian tubes include target or beaked appearance (echogenic mass with multiple concentric hypoechoic stripes)/snail-shell appearance/an enlarged hypoechoic or echogenic mass/ellipsoid or tubular mass with heterogeneous internal echoes
Other appearances of the twisted pedicle with/without fallopian tubes include solid amorphous/target-like/beaked or serpentine-like protrusion extending from the uterus and partially covering the adnexa
Eccentric wall thickening leading into thickened tubes suggests haemorrhagic infarction
Ovarian tenderness on transducer pressure – not elicitable on other modalities
Ipsilateral deviation of the uterus
Abnormal location of the ovary at or near the midline, superior to the uterine fundus or on the contralateral side. ‘Double bladder’ sign if midline location.
Abnormal placed ovary at or near the midline with far anterior or posterior location, or on the contralateral side
Engorged vessels on the ipsilateral side distal to the torsion
Periadnexal fat infiltration
Poor to absent adnexal enhancement – necrosis
DOPPLER
• Reduced or absent ovarian venous flow
• Reduced or absent ovarian arterial flow – is usually associated with abnormal venous flow
• Swirling appearance of vessels within a twisted vascular pedicle
• Absence of reversal of diastolic flow in the ovaries
• Lack of flow within the twisted vascular pedicle and absence of central venous flow within the ovaries – favours nonviability
• Normal arterial or venous flow within the ovaries does not exclude torsion – this may be due to intermittent torsion (with the imaging performed during the stage of detorsion) or be related to dual arterial supply to the ovaries
11.16.2
BENIGN OVARIAN LESIONS
K. Geetha
Introduction
Benign ovarian lesions are commonly seen in day-to-day practice and may be incidentally seen or diagnosed in symptomatic patients by imaging techniques. Imaging characterization of an ovarian lesion is significant to plan the management. Ultrasound is the first-line imaging modality in evaluating ovarian lesions. Both transabdominal and endovaginal ultrasound should be done to rule out the lesion. Magnetic resonance imaging (MRI) may be valuable for the further characterization of few benign ovarian lesions if ultrasound is equivocal. In this topic, we classified benign ovarian lesions into four groups based on morphological appearance and described the imaging features in ultrasound, computed tomography (CT) and MRI.
Approach to benign ovarian lesions
Optimal assessment of benign ovarian lesions often need multidisciplinary approach, which will be based on clinical history, physical examination, serum markers and imaging techniques. As some benign and malignant ovarian lesion have overlapping or similar imaging features, multidisciplinary approach, such as clinical history, serum markers and imaging techniques, helps to derive the probable diagnosis. It is important to diagnose the type of benign ovarian lesions as it changes the patient management. Certain lesions such as endometrioma, mature cystic teratoma and paraovarian cysts have to be diagnosed since they affect patient’s fertility and sometimes can lead to torsion of ovary.
Clinical history such as reproductive age, infertility, dysmenorrhea in cases of endometriosis and ovulation induction for ovarian hyperstimulation syndrome are important. The most commonly used serum tumour marker for epithelial tumours is cancer antigen (CA)-125. In postmenopausal women, CA-125 is highly sensitive and specific but it has less specificity in premenopausal women as it is elevated in other benign conditions.
Imaging has significant role in detection, characterization of benign ovarian lesions. Ultrasound, colour Doppler MRI are useful in characterization of benign ovarian lesions. CT helps to identify lesions containing fat tissue and calcifications, like mature teratoma.
Imaging features in general suggestive of benignity are size less than 4–7 cm, thin regular wall (<3 mm) unilocular or multilocular cysts with no internal septations, papillary projections or solid components and no vascularity, resolution of lesion in 6–12 weeks in follow-up imaging.
Classification of benign ovarian lesions based on morphological appearance (Table 11.16.2.1)
Brenner tumour, fibrothecomas, fibromas and thecomas.
Imaging findings
1. Unilocular cyst
1.1 Follicular cyst: After ovulation, failure of involution of Graafian follicle causes follicular cyst measuring >3 cm.
Haemorrhagic cyst: If bleed occurs within the ovarian cyst, it produces low-level echoes within the cyst in ultrasound. On colour Doppler, there will be no internal vascularity.
1.2 Corpus luteum cyst: A corpus luteum may seal and fill with fluid or blood, forming a corpus luteum cyst. USG shows complex ovarian cyst with wall vascularity on colour Doppler. This complete circular vascularity on Doppler imaging is called the complete ‘ring of fire’ appearance.
1.3 Polycystic ovary syndrome (PCOS) affects approximately 20% of premenopausal women and is one of the most common endocrinopathies of women.
The classic triad of PCOS is:
1. Oligomenorrhoea
2. Hirsutism
3. Obesity
The diagnosis of PCOS requires any two of the following three criteria:
1. Ovulatory dysfunction (either oligoovulation or anovulation)
2. Clinical and/or biochemical features of hyperandrogenism
3. Polycystic ovarian morphology on ultrasound
PCOS is typically characterized by small-sized follicles than seen in normal ovaries. USG demonstrates peripherally arranged 10 or more follicles whose diameter is about 2–8 mm around the central stroma, which is hyperechoic. Stroma/area (S/A) ratio of greater than 0.34 (calculated as ovarian stromal area to the total area of the ovary has 100% sensitivity and specificity in detecting PCOS.
US features: Rotterdam criteria
(a) One or both ovaries demonstrate 12 or more follicles measuring 2–9 mm in diameter – peripherally arranged with central echogenic stroma – ‘string of pearls’ appearance.
(b) The ovarian volume more than 10 cm3.
(c) Only one ovary meeting either of these criteria is sufficient to establish the presence of polycystic ovaries.
MRI shows enlarged ovaries with central stroma which is hypointense on T2 and multiple peripherally arranged small follicles.
1.4 Ovarian hyperstimulation syndrome is a relatively rare condition which is bilateral as it occurs due to overstimulation by human chorionic gonadotropin (hCG). Hormonal overstimulation can occur in gestational trophoblastic disease, PCOS or in patients receiving hormonal therapy. When they occur in normal pregnancies, they tend to resolve spontaneously after birth. Molar pregnancies, erythroblastosis foetalis are associated with hyperstimulation. On USG, there will be bilateral enlargement of ovaries with multiloculated cyst replacing the complete ovary. Clinical history of hormone stimulation helps in arriving at the diagnosis (Fig. 11.16.2.1).
1.5 Serous cystadenoma presents as a unilocular cystic benign lesion with thin regular wall. Wall thickness is <3 mm. The lining is flat without any internal septations, solid components or papillary projections. They usually show no significant contrast enhancement. Serous fluid is hypointense on T1-weighted and hyperintense on T2-weighted images (Fig. 11.16.2.1). They are more often bilateral (12%–23%) and smaller than mucinous cystadenomas (Fig. 11.16.2.2).