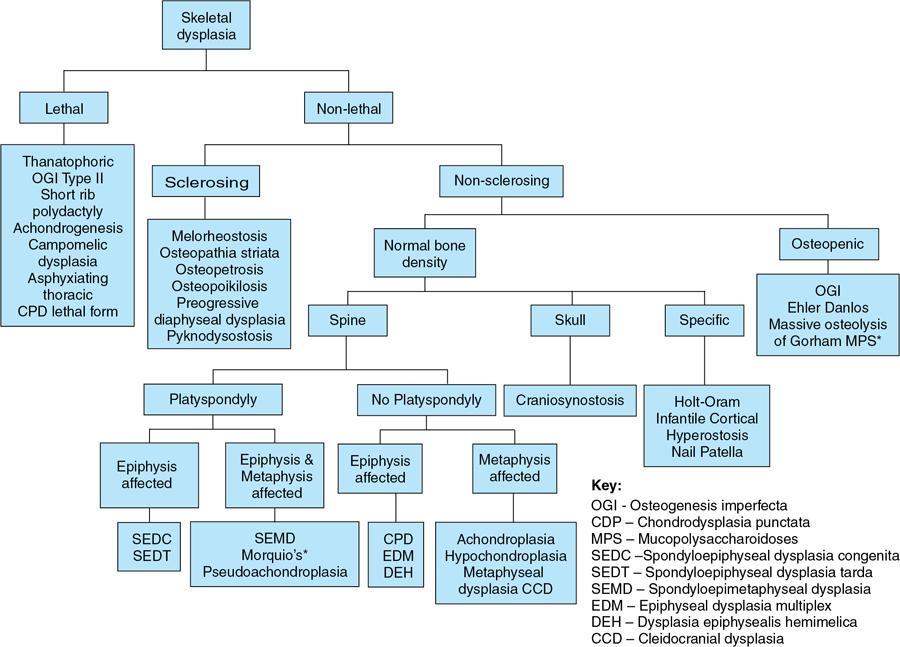
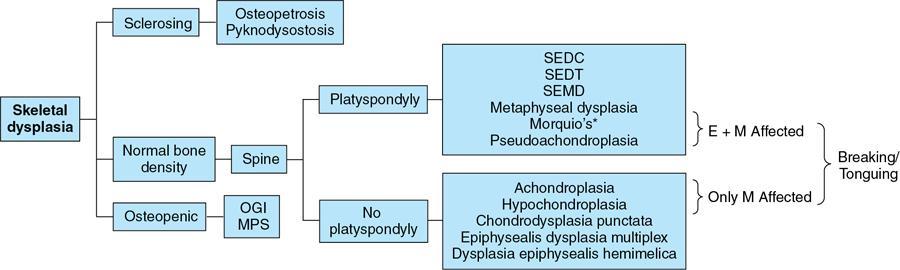
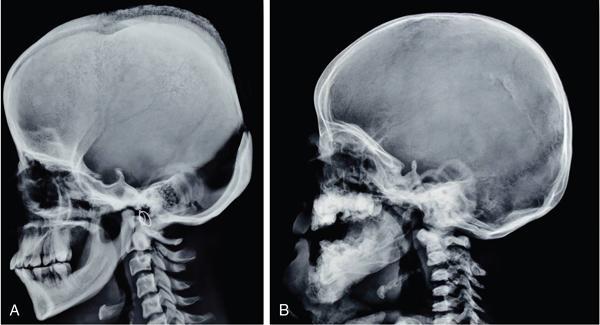
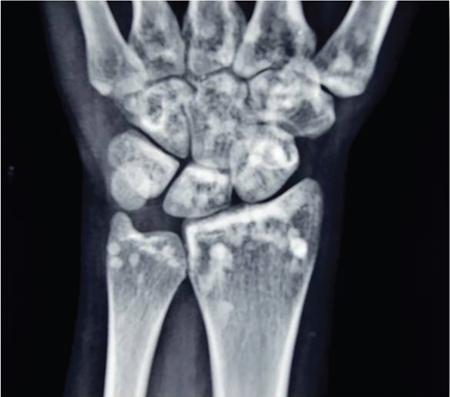
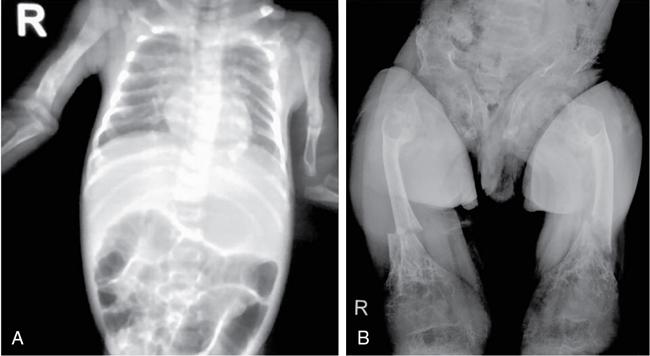
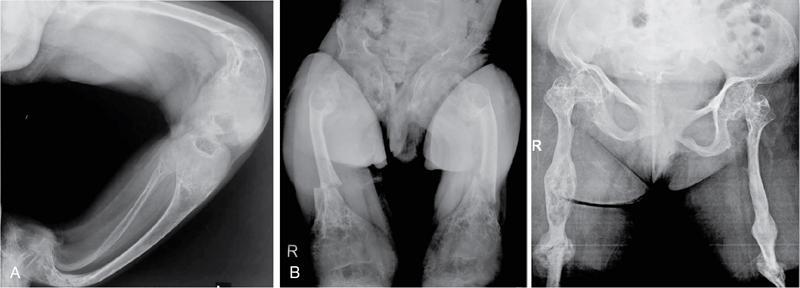
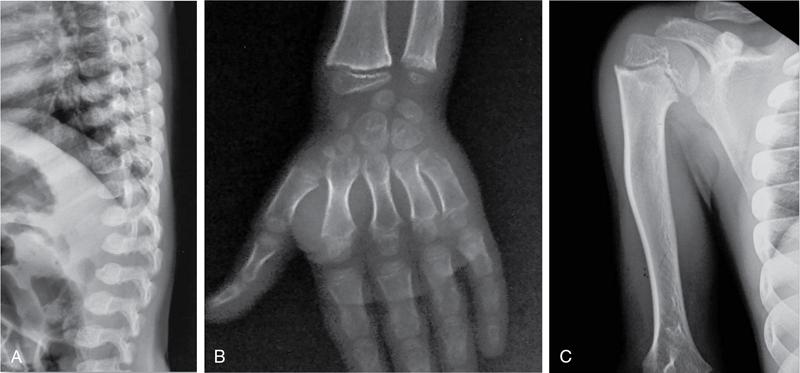
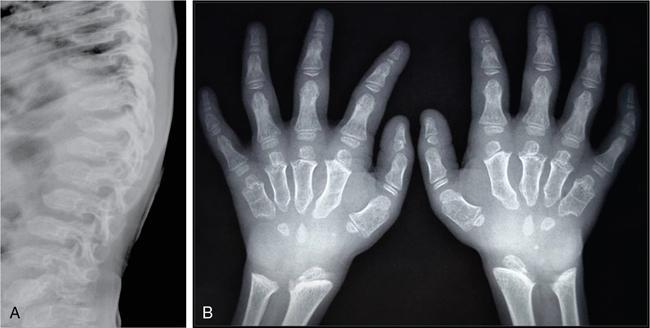
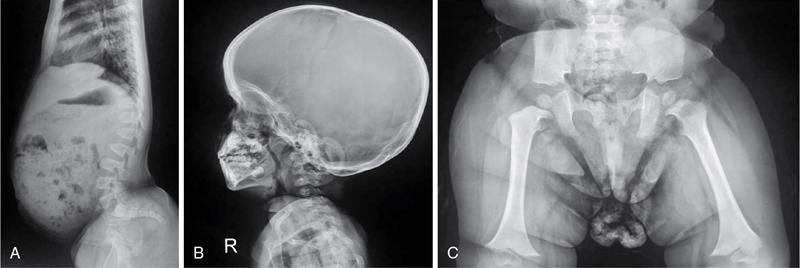
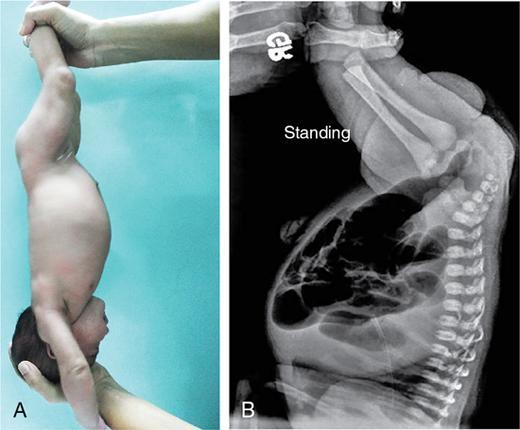
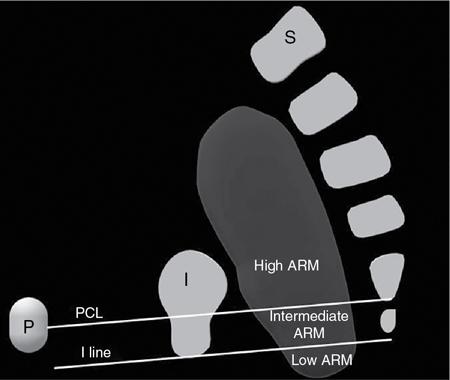
MISCELLANEOUS PAEDIATRIC RADIOGRAPHY – TECHNIQUES AND INTERPRETATION: SKELETAL SURVEY Padma V. Badhe The skeletal survey, generally performed in children, is a set of radiographs done in order to evaluate the entire skeleton. A skeletal survey, commonly used to evaluate skeletal dysplasias, acquired metabolic disorders and suspected child abuse, is still the key radiological investigation for the same. Hence, an explicit understanding of the technique along with the common disorders forms the basis of making a diagnosis in these paediatric pathologies. A skeletal survey is done for various skeletal dysplasias, non-accidental injury (battered baby syndrome) and suspected child abuse. It can also be done in cases of metabolic bone diseases, disseminated infections, multiple myeloma, eosinophilic granuloma. It is also used in evaluation of metastatic bone diseases and polyarticular arthropathy. Orthogonal views of the skull, spine, pelvis and one extremity are taken, preferable in standing position. For preterm babies/newborns, AP and lateral views of babygram may be taken. Projections: For skeletal dysplasias: Additional views: Both extremities may be taken if epiphyseal abnormalities and limb asymmetry is present. Focused views for specific pathologies may be taken. When a diagnosis remains uncertain, 1 year follow up is usually recommended. For preterm babies/newborns: AP and lateral views of babygram may be taken with additional specific views for extremities. For suspected non-accidental injury (NAI): AP and oblique view of chest is taken for better evaluation of the ribs. AP view of abdomen with pelvis. Both upper and lower limbs are evaluated. In lower limbs, two projections in AP and lateral (one with both femur including hip and knee joints; and another for foot and ankle) is taken. AP and lateral views of whole spine, skull. Oblique view of hands. A babygram should be avoided in cases of NAI, as subtle fractures are easily missed. Proper legal documentation while taking the views is very important and ideally two health care professionals must be present. For metabolic disorders: entire skeletal survey is usually not required. Specific views of hands, knees and spine may be taken with additional views depending on the suspected pathology. Centring point: Varies according to the part being examined. Angulation, collimation and orientation: Varies according to the part being examined. Images must be well collimated to obtain lower radiation dose. Detector size: Varies according to the part being examined: 8″ × 10″, 10″ × 12″, 11″ × 14″. Exposure: Ideally high kVp images are taken to reduce radiation dose. But in suspected NAI, low kVp/high mA images are recommended to better demonstrate findings. SID (Source Image Distance):100 cm Grid: Grids are not routinely used to image spine, pelvis, skull and abdomen in children. Radiation dosage: 0.3–3 mSv Essential image characteristics: Adequate spatial resolution, high signal to noise ratio, low kVp (50–70) for high contrast should be done. Excellent bone and soft tissue details are required. The presentation of skeletal dysplasia can range anywhere from minimal stunting of growth and bowing of limbs to severe dwarfism and multiple fractures. Knowledge of the commonly encountered dysplasias with an approach to arrive at a diagnosis is vital in any Radiologist’s practice The following flow chart summarizes the classification of important skeletal dysplasia: The following table summarizes the various dysplasias affecting the axial skeleton: TABLE 7.5.1.1 The following flow chart summarizes the working approach to skeletal dysplasias: Osteopetrosis (Albers-Schonberg disease/Marble bone disease) (Fig 7.5.1.1): Osteopetrosis clinically presents with anaemia/thrombocytopenia or cranial nerve compression. Radiological features include generalized increase in bone density with loss of medullary space. However, cortico-medullary appreciation with cortical thinning is also rarely seen. Bone within bone appearance with Erlenmeyer flask deformity is also noted. Pyknodysostosis (Figs. 7.5.1.2 and 7.5.1.3): patient presents with short stature. Unlike osteopetrosis, there is no anaemia. Radiographs show generalized increase in bone density with preserved medullary canal. There is mandibular hypoplasia with obtuse angle. Acro-osteolysis is also a feature. Dental caries with osteomyelitis of the jaw may be seen. Sclerosing dysplasia presenting as wavy undulating new bone formation. Usually monomelic, lower limb and along one side. The classic appearance is described as Dripping candle Wax sign. It is a Sclerosing dysplasia with radiological features of symmetric juxta-articular involvement in epimetaphyseal region. They are 1–10 mm in diameter and uniform in size. No metabolic activity is seen on bone scans. This skeletal dysplasia shows diffuse decrease in bone density with paper-thin cortex. Fractures heal in normal time but shows callus with poorly cellular matrix. Wormian bones and enlarged sinuses may be seen. Codfish vertebra (Biconcave vertebra) may be seen. Metaphyseal corner fractures are not seen in osteogenesis imperfecta that helps to differentiate it from battered baby syndrome. There are four types of OI out of which type one is most common (Figs. 7.5.1.6 and 7.5.1.7). The radiological features of MPS include Osteopenia and Universal platyspondyly. The intervertebral disc spaces are maintained. Proximal pointed metacarpals is an important radiological finding. Hurler’s syndrome show anteroinferior beaking with short and wide metacarpals. Varus deformity of humerus is characteristically seen in Hurler’s syndrome (Fig. 7.5.1.8). Mental retardation & corneal clouding is seen in Hurler’s syndrome whereas these Hunter’s disease has normal intelligence with no corneal clouding. Morquio’s syndrome shows central beaking (Fig 7.5.1.9). This skeletal dysplasia shows normal bone density with rhizomelic limb shortening and normal trunk. Narrowing of spinal canal is classically seen with decrease in the Interpedicular distance caudally. Other radiological features include trident hand (separation of middle & third fingers), Champagne glass pelvis (short, flat ilia and small sciatic notch), bullet nose vertebra and overexpansion of skull with narrow foramen magnum (Fig. 7.5.1.10). This skeletal dysplasia is characterized by normal bone density with dwarfism and normal craniofacial skeleton. The interpedicular distance is normal. There is severe platyspondyly with anterior tonguing (disappears at older age). Other radiological features include increased disc space, short stubby metacarpals, small irregular epiphysis and widened metaphysis. Anterior tonguing is a feature of Pseudoachondroplasia. This form of skeletal dysplasia involves the spine and epiphyses (Fig. 7.5.1.11). There is normal bone density with rhizomelia. Spine and Pelvis can be involved. Premature osteoarthritis can be seen. The other characteristic features include Platyspondyly and small irregular epiphysis. There are two forms Spondyloepiphyseal dysplasia Congenital and Spondyloepiphyseal dysplasia Tarda. Spondyloepiphyseal dysplasia Congenita is Autosomal dominant and shows pear-shaped vertebrae. Spondyloepiphyseal dysplasia Tarda is X Linked recessive with heaped up vertebrae. It has two forms. The first form is Conradi Hunermann syndrome which is autosomal dominant characterized by asymmetric limb shortening with metaphyseal flaring (Fig. 7.5.1.12). The Autosomal recessive form is Fatal in first few years. Rickets: Rickets refers to deficient mineralization of the growth plate in the paediatric population due to deficiency of vitamin D. In an immature skeleton, there is abnormal mineralization at the zone of provisional calcification in the metaphysis due to osteoid deposition resulting in widening of the growth plate. The features of rickets include fraying, splaying and cupping (Fig. 7.5.1.13). Fraying denotes indistinct margins of the metaphysis whereas splaying denotes widening of metaphyseal ends. Term ‘Cupping’ is used for increased concavity of the metaphysis. These findings are typically seen involving areas of active growth (e.g. distal femur and proximal tibia in the knee) Bowing is a result of associated osteomalacia leading to weakening of weight-bearing lower limb bones. Other bone deformities such as genu valga, genu varum, protrusio acetabuli can also be seen. The lower ribs may also be drawn inwards inferiorly by the attachment of the diaphragm this is called Harrison’s sulcus. Scurvy: Scurvy is a result of dietary deficiency of Vitamin C (ascorbic acid). The classic presentation is that of a patient with an increased bleeding tendency and osteopenia with poor wound healing. Features of scurvy include generalized osteopenia with cortical thinning termed as ‘pencil-point’ cortex. Other radiological findings include the periosteal reaction due to subperiosteal haemorrhage. Expansion of the costochondral junctions occurs forming scorbutic rosary. Bleeding into the joint spaces may result in hemarthrosis. Circular, opaque radiologic shadow surrounding epiphyseal centres of ossification may result from bleeding (Wimberger ring sign) (Fig. 7.5.1.14). Frankel line may be seen. It represents dense zone of provisional calcification. Lucent metaphyseal band is seen underlying Frankel line called as Trümmerfeld zone. Metaphyseal spurs may be seen that result in cupping of the metaphysis (Pelkin spur). Pelkin fracture (metaphyseal corner fracture) can also be seen. Images obtained must be of good resolution with adequate bone and soft tissue details. Additional views: They have already been described in positioning. CT Brain in can be done in cases of NAI to look for subdural hematomas. A skeletal survey is the first-line imaging modality for evaluation of skeletal dysplasia, nonaccidental injury and metabolic bone diseases. The skeletal survey must be tailored according to the respective indication. It helps to characterize syndromic patterns in skeletal dysplasias, with evaluation of complications. In cases of diagnostic dilemmas, additional focused view and occasionally yearly follow-up is recommended. A high index of suspicion is needed in utilizing skeletal survey as a diagnostic modality in NAI. At the same time, one must also remember the legal and social implications of making this diagnosis. BABYGRAM Babygram is a colloquial term used for a radiograph of the whole body of a newborn or just the chest and abdomen (thoracoabdominal babygram) on a single image. As the name suggests it is a rather non-targeted study. It is most commonly requested after line placement. Evaluation of skeletal abnormalities in a deceased foetus is typically performed using anteroposterior and lateral views of a babygram. It helps in pointing out skeletal causes of death in stillborn or dead foetuses. This will help the treating physician and parents understand the reason for baby’s death. This will also help in future genetic counselling of the couple. Sometimes chest or abdominal radiographs of the baby are requested but due to radiographers error or inexperience with small babies, there is inclusion of the region not to be assessed leading to a false babygram. Babygram is most frequently done after line placement in neonates, to view the position of the umbilical vein or artery catheter and to confirm appropriate placement. It is a useful modality in skeletal dysplasias (Fig. 7.5.1.15) like osteogenesis imperfecta, thanatophoric dysplasia and chondrodysplasia punctata. It can also be used for skeletal deformations probably caused by foetus akinesia and in cases of Caudal regression syndrome. In stillborn foetuses, it is used for evaluation of skeletal dysplasias prior to an autopsy (Fig. 7.5.1.16). It is also used in screening for surfactant deficiency and in cases of Necrotizing Enterocolitis in preterm babies where it can help to see the bowel dilatation, intramural and portal venous gas. It can be done in aneuploidies like trisomy 18 and in cases of sudden infantile death syndrome. All the essential equipment and room need to be prepared including the exposure factor. This should be done prior to placing the baby on the table to prevent any neonatal heat loss. Ensure that the baby is correctly identified. Give brief explanation to the patient’s parents regarding the procedure, its risks and benefits. Ensure that the accompanying relative is not pregnant (if female). Parents/guardians/nurses should be instructed to hold the baby with arms above the head and legs straight down. Sandbags/tapes can be used to immobilize the baby. Avoid taking the radiograph when baby is crying. Normal appearance: The endotracheal tube should lie in the lower third of trachea, distance can vary with position of baby’s head. Umbilical artery catheter has an inferior dip along the internal iliac artery, which then turns superiorly along the aorta. The tip should lie in the mid-thoracic aorta (T6–T10) or lower (L3–L4) away from aortic branches to prevent any thrombosis. Umbilical venous catheter does not have the inferior curvature, but rather a posterolateral angulation to the right near the liver through the ductus venosus. The tip should lie in the superior IVC or right atrium at T8/T9 vertebral level (Fig. 7.5.1.17). Portal venous gas may be seen initially after insertion. In a stillborn foetus, the approximate gestation age of the foetus and corresponding ossification centres must be known. In early gestation, the lack of appearance of an ossification centre may be mistaken for skeletal dysplasia. Both chest and abdomen should be included. In a rotated patient, the distance between the spinous process to medial end of clavicles will be asymmetric. The medial end of clavicle should overlap the lung apex, if above, suggests lordotic image. Motion artefacts to be reduced as much as possible. A crying neonate may result in an expiratory film, and hence must be evaluated accordingly. In evaluation of skeletal dysplasias in the newborn, additional views of skull and hand have to be obtained. Baby gram is a useful diagnostic investigation for position of the paediatric umbilical catheters. It helps in general survey in skeletal dysplasia (Fig. 7.5.1.18). It is a simple, effective study in deceased foetus for diagnosis and further counselling, sometimes obviating the need for an autopsy. As baby gram is a non-targeted study, it increases the dose of radiation for the baby. As the exposure settings remain same for the entire body of the baby, the quality of the image decreases. This increases the chances of missing subtle findings. The babygram in a neonate is currently used to localize umbilical catheters. In stillborn fetuses, it is still an important study for documenting and confirming skeletal dysplasias. Understanding the normal appearance as per gestation age and patterns of various common skeletal dysplasias is essential for evaluation. Being a non-targeted study, it should not be used as an alternative study to evaluate the chest or abdomen considering radiation exposure and poorer image quality. INVERTOGRAM Invertogram was first described by Wangensteen and Rice in 1930. It was used as a first investigation to be ordered in evaluation of infants with clinically diagnosed or suspected Anorectal Malformation (ARM). ARM is a serious but surgically treatable congenital malformation with approximate incidence of 1 in 5000 live births. Though the diagnosis of this condition is based on clinical history and physical examination, imaging plays an important role in deciding the type of ARM, and associated complications to aid in management. International classification of anorectal malformations is as follows. Syndromic association is seen as a part of VACTERL defects, trisomy 21 13 and 18, Klippel Feil syndrome, cat eye syndrome etc. The main indication of Invertogram is to evaluate anorectal malformation in a neonate. A radio-opaque marker is placed over the external anal opening. Infant is held inverted by holding both thighs, maintaining this posture for at least 5 minutes before taking an X-ray in true lateral position (Fig. 7.5.1.19). Exposure is made during inspiration. The Invertogram should ideally be done 24 hours after birth as, the rectal gas may not reach the terminal segment if study is done too early. Pubo-coccygeal line (PCL) is drawn from upper border of pubic symphysis (which corresponds to centre of pubic bone on lateral X-ray) to sacrococcygeal junction. I point is the inferior most point of ischial ossification centre. A line which is drawn parallel to PC line passing through the I point is called I line. ‘A’ point is represented by marker placed at anal pit. The position of rectal pouch gas shadow is observed with respect to these lines and appropriate diagnosis is made (Fig. 7.5.1.21). A diagnosis of high ARM is made when gas shadow of rectal pouch is cranial to PCL. If rectal pouch gas shadow is in between PCL and I line, it is called as intermediate ARM and if it is caudal to I line, it is diagnosed as low ARM. Gas in urinary bladder or vagina or beaking of gas shadow of rectal pouch indicates fistula into one of these sites. Associated congenital abnormalities like spinal defects are also looked for in the invertogram (Fig. 7.5.1.22). Invertogram done too early (less than 24 hours) may not demonstrate rectal gas. Meconium plugging the terminal segment gives false position of the rectal gas. Positioning can cause discomfort to child and an irritated crying child actively contracts the sphincter muscles, pushing the gas shadow higher. Rectum may be pulled cephalad due to gravity in inverted position. The rectal gas may escape through an associated fistula. Erroneous interpretation can also occur due to sacral anomalies and when gas in vaginal cavity is misinterpreted as distal rectal gas. Both ischial bones should superimpose and terminal blind loop should be well distended. It is an easily available modality and can be done quickly, does not require additional equipment. It has lesser radiation dose as compared to CT invertogram. It provides a rough guide as to the type of ARM and decides management. Higher localization of obstruction due to various causes like meconium plugging, imaging done too early etc. as described above in pitfalls. It is more uncomfortable to the baby as compared to the prone cross-table lateral view, and a crying baby contracts the puborectalis leading to erroneous results. K. L. Narasimharao et al. modified the technique and proposed cross-table lateral view for evaluation of infants with ARM’s which has shown equal or better information and has now replaced invertogram (Fig. 7.5.1.23). Prone cross-table lateral view is considered equivalent or even better in determining the level of anomaly. Positioning is in this view is prone in genupectoral position (at least for 3 minutes). It is taken in true lateral and during inspiration. The lines used to delineate types of ARM is essentially the same as in an invertogram. It is preferred over invertogram as relatively easy positioning of the infant and less discomfort allows for better cooperation of neonate during the study. It also eliminates the effect of gravity. ARM with fistula is better delineated as, in an invertogram, fistula/gas is at the highest level and gas may escape through it. CT invertogram is another modality that delineates anatomy better but is rarely used. In the era of cross-section imaging, MRI and USG have opened new modalities for accurate diagnosis of ARM, but invertogram being readily available, inexpensive, quick and cost-effective is used as first investigation for evaluating a patient with suspected or confirmed case of ARM. Cross-table lateral view has replaced invertograms as it is more patient-friendly and equally effective. UPPER GASTROINTESTINAL SERIES Rushit S. Shah An upper gastrointestinal (GI) study is a radiographic examination of the GI tract from the pharynx to the ligament of Treitz after oral administration of contrast agent. The use of upper GI studies is gradually declining with the increasing availability of paediatric endoscopy and the challenge for the modern radiologist to work in conjunction with the surgeon and gastroenterologist to select the right patients for an upper GI series. However, the upper GI series remains the key for demonstrating many anatomical abnormalities. The upper GI series is also useful in evaluating gastro-oesophageal reflux in conjunction with 24 pH monitoring. The upper GI examination is useful in evaluating many conditions including but not limited to:
7.5: Paediatric imaging techniques of abdomen and pelvis
Introduction
Indications
Patient positioning
Technical factors
Pathologic appearance
Locations
Examples
Skull
Achondroplasia, cleidocranial dysplasias
Mandible
Pyknodysostosis
Clavicle
Cleidocranial dysplasia
Ribs
Asphyxiating thoracic dysplasia, Thanatophoric dysplasia
Spine
Spondyloepiphyseal dysplasia congenita, Mucopolysaccharidoses
Pelvis
Achondroplasia


Melorheostosis (leri type of osteopetrosis)
Osteopoikilosis
Osteogenesis imperfecta (lobstein’s disease)

Mucopolysaccharidoses
Achondroplasia
Pseudoachondroplasia
Spondyloepiphyseal dysplasia (SED)

Chondrodysplasia punctata

Metabolic disorders


Image technical evaluation
Take-home message
Introduction
Indications


Patient positioning
Technical aspects
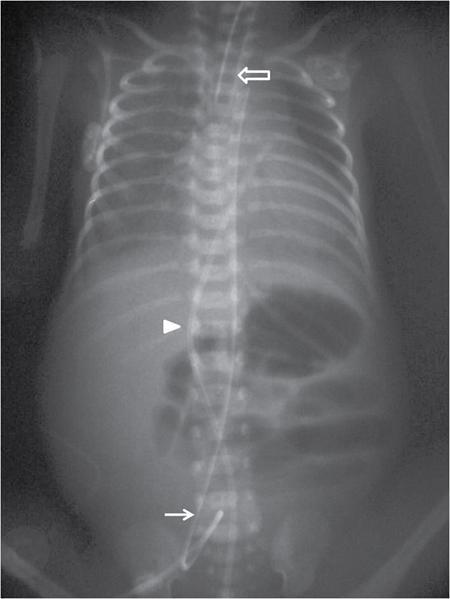
Image technical evaluation
Advantages

Disadvantages
Take-home message
Introduction
Indication
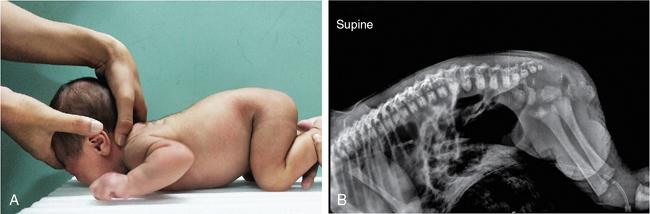
Patient positioning
Technical factors
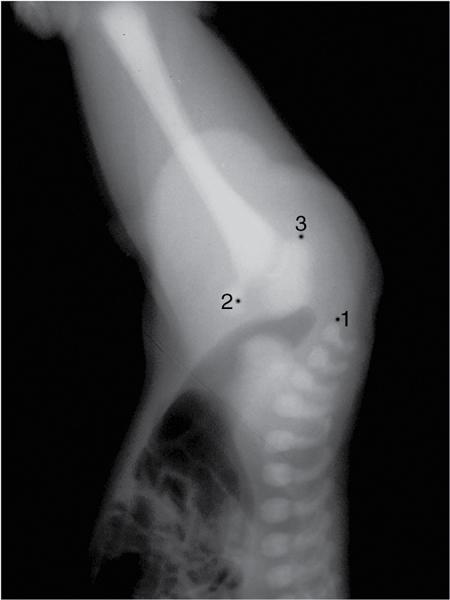
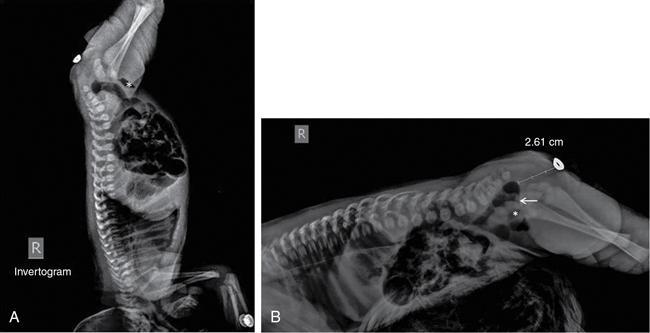
Normal appearances and variants
Essential image characteristics (Fig. 7.5.1.20)
Pathological appearances
Pitfalls
Image technical evaluation
Advantages
Disadvantages
Alternate views
Take-home message
Introduction
Indications
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


