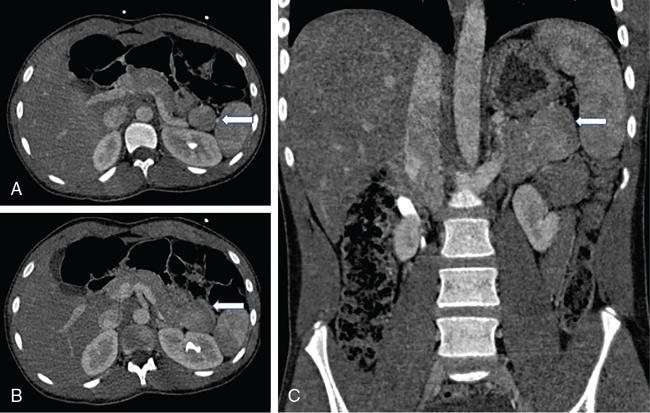
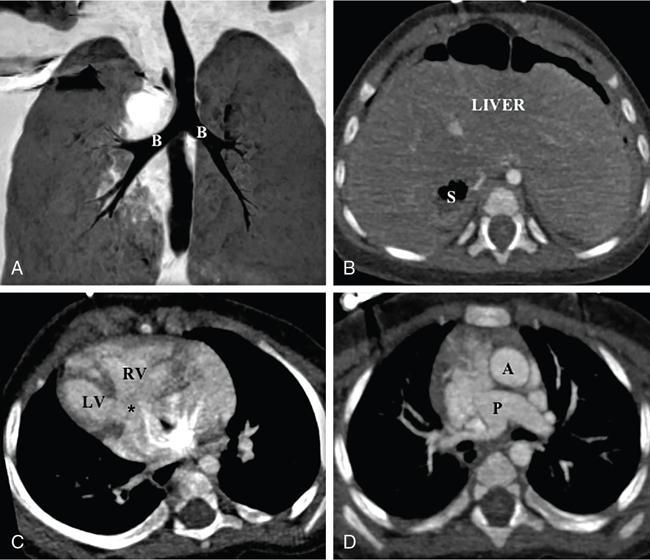
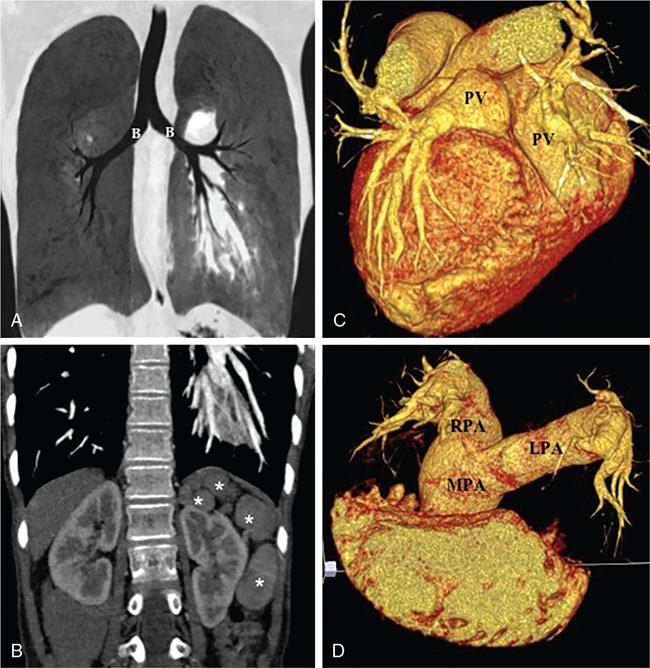
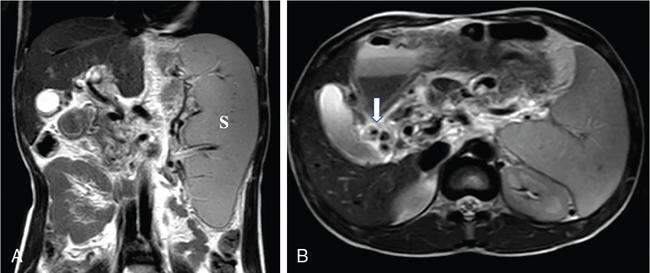
Kalpana Bansal, Poonam Narang The paediatric splenic abnormalities include both congenital and acquired pathological conditions. The congenital anomalies include variations in splenic number, location or fusion abnormalities and are more common than the acquired pathological conditions like splenomegaly, focal lesions, tumours and trauma. The splenic pathology can be evaluated with a wide variety of available imaging modalities including an ultrasound that is usually the first modality of choice in paediatric patients, computed tomography, magnetic resonance imaging and technetium-99m scintigraphy. The pattern-oriented approach to the radiological evaluation of splenic abnormalities may help to reach an accurate diagnosis and plan patient management. The congenital anomalies are common splenic abnormalities in paediatric patients. They usually result from absent or incomplete fusion of splenic lobules into one single organ before birth or abnormal location of the spleen. The congenital malformations include: The accessory spleen is commonly referred to as the splenunculus or supernumerary spleen. It results from the failure of the fusion of the primordial splenic buds in the dorsal mesogastrium during foetal life. The incidence is seen in 10%–30% of the population. The most common location of an accessory spleen is near the splenic hilum seen in about 75% of the cases and the pancreatic tail in 25% cases. It may be located anywhere along the course of the splenic vessels or in the abdomen and pelvis. The size of an accessory spleen ranges from few millimetres to centimetres and the number may vary from 1 to 6 (Fig. 9.21.1). The accessory spleens are usually asymptomatic and incidentally detected on imaging. But an accessory spleen present in an unexpected location can be misinterpreted as an abnormal soft tissue mass or lymph node. The characteristic imaging findings of the accessory spleen include similar imaging appearance to normal spleen on CT and MRI. The demonstration of feeding artery from the splenic artery can also be helpful in the differential diagnosis. Iron-containing MR contrast agents and Tc-99 sulphur colloid scintigraphy may be useful to confirm the diagnosis. The clinical significance of accessory spleen is seen in patients who had splenectomy for hypersplenism. In such patients, the accessory spleen may hypertrophy and result in recurrent disease; however, in patients of splenic trauma who had a splenectomy, it may help preserve the immune functions of the spleen. Splenopancreatic fusion is a rare anomaly that results due to abnormal fusion of splenic or pancreatic tissue as both organs arise from the dorsal mesogastrium close to each other. The ectopic splenic tissue may be located in the pancreatic tail (Fig. 9.21.2) and ectopic pancreas in the spleen or accessory spleen. It is also an incidental finding and asymptomatic. The clinical importance is to avoid complications during splenectomy or distal pancreatectomy. Splenogonadal fusion is an extremely rare anomaly that results due to the persistence of splenic tissue between the spleen and left testicle or epididymis. It may simulate masses and warrant unnecessary surgeries. The demonstration of splenic tissue connecting the spleen with the left gonad using any of the imaging modality helps in definitive diagnosis. Wandering or ectopic spleen is an extremely rare entity that results due to laxity or maldevelopment of the supporting splenic ligaments, and spleen can be found in any part of the abdomen. The incidence in several large studies of splenectomy is less than 0.5% and is mainly seen in children. The wandering spleen may be detected incidentally or present with different degrees of abdominal pain related to intermittent or acute torsion of the vascular pedicle. Ultrasound and CT remain the mainstay of diagnosis. Imaging findings include the absence of spleen in its normal position and a mass located anywhere in the abdomen or pelvis showing imaging and enhancement characteristics of normal splenic tissue. Besides, in the case of torsion, a typical ‘whirl’ pattern of the twisted pedicle and altered enhancement may also be demonstrated. Doppler shows absent flow within the spleen and low diastolic velocity with raised resistive index in the proximal splenic artery. The unenhanced CT shows hypoattenuation of the spleen, hyperdense intraluminal thrombus in the splenic artery and high density of the splenic capsule relative to parenchyma (‘rim’ sign). The contrast-enhanced CT shows absent or heterogeneous enhancement. The treatment modality of choice is splenopexy; however, splenectomy may be indicated in cases of infarction. Polysplenia and asplenia are typically seen in association with situs ambiguous or heterotaxia. Situs ambiguous with asplenia also known as Ivemark syndrome refers to right isomerism or bilateral right-sidedness and is characterized by an ambiguous location of abdominal organs with congenital absence of the spleen. It is more prevalent in males and associated with congenital heart disease in almost all cases (Fig. 9.21.3). Most patients die within the first year of life due to associated severe congenital heart disease and immunodeficiency due to absent spleen. Situs ambiguous with polysplenia is referred to as left isomerism or bilateral left sidedness. It is more common in females. The spleen may be located on the left or right side of the upper abdomen, the number may vary from 2 to 6 and diameter ranges from 1 to 6 cm (Fig. 9.21.4). The coexisting anomalies include a right-sided stomach, a midline or left-sided liver, bowel malrotation, short pancreas, absent gallbladder and associated inferior vena cava anomalies. Splenosis is an acquired anomaly that occurs following splenic trauma or splenectomy. It results due to auto-transplantation of splenic tissue usually in the peritoneal cavity but also may occur in extraperitoneal locations like the thoracic cavity. Splenosis is usually asymptomatic and incidentally detected on imaging. Splenosis is an acquired condition so it has distorted architecture and is supplied by surrounding vessels so, it can be mistaken for neoplastic lesions and lead to unnecessary surgery. A patient who had splenectomy for hypersplenism, splenosis may result in recurrent disease. However, a functioning splenic tissue may be required to preserve normal immunological function and remove old blood cells. Splenomegaly is a nonspecific finding seen as a manifestation of various disease processes listed in Box 9.21.1. CAUSES OF SPLENOMEGALY Ultrasound is usually the first and useful modality to evaluate enlarged spleen. It accurately measures the splenic span and also assesses the splenic echotexture, homogeneous or heterogeneous. Doppler USG is very good for the assessment of portal hypertension as a cause of splenomegaly by demonstrating flow in the splenoportal axis and collaterals. Both USG and CT also assesses the ancillary findings like lymphadenopathy in case of lymphoma or tuberculosis. Portal hypertension is one of the most common noninfectious causes of splenomegaly in children. Patients usually present with significant gastrointestinal bleed or massive splenomegaly. The causes of portal hypertension may be prehepatic, intrahepatic or posthepatic. The portal vein thrombosis is mostly idiopathic in children and results in collateral vessel development at porta known as cavernous transformation of the portal vein or portal cavernoma and portosystemic collaterals with massive splenomegaly (Fig. 9.21.5).
9.21: Paediatric splenic abnormalities
Introduction
Congenital malformations
Accessory spleen and fusion anomalies
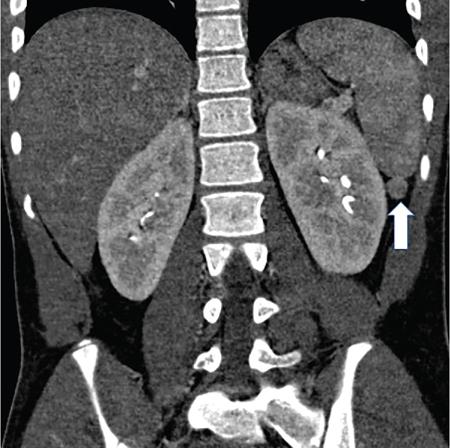
Wandering spleen
Polysplenia and asplenia
Splenosis
Splenomegaly
Portal hypertension.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


