Fig. 12.1
Pancreatic metastasis from renal cell carcinoma. A 61-year-old female with past medical history of renal carcinoma that was treated 16 years earlier with right nephrectomy. Patient was complaining of abdominal discomfort. CECT axial images (a, b) show a heterogeneous, hypervascular mass in the body of the pancreas (arrows). Intraoperative ultrasound gray scale (c) (arrow) and color Doppler (d) transverse scans show a well-circumscribed hypervascular, hypoechoic pancreatic mass. Photograph of the gross specimen reveals a round, solid, encapsulated mass with light brown parenchyma with areas of hemorrhage (e) (arrows). Histology of the mass (f) (H&E, 50×) demonstrates a tumor composed of large cells with clear cytoplasm arranged in a nesting/acinar pattern, consistent with metastatic renal carcinoma, clear cell type
Fig. 12.2
Pancreatic metastasis from renal cell carcinoma associated with pancreatic duct dilatation. A 53-year-old with past medical history of renal cell carcinoma that was treated 3 years earlier with right nephrectomy . CECT axial images (a, b) demonstrate a small hypervascular small mass in the body of the pancreas (arrows) associated with dilatation of the distal pancreatic duct (arrowheads). Intraoperative ultrasound gray scale (c) and color Doppler (d) images demonstrate a small hypoechoic, hypervascular pancreatic mass (arrows) associated with dilatation of the pancreatic duct. The patient underwent a Whipple procedure. Gross image of the resected specimen (e) shows a small, round, yellow mass in the head/neck of the pancreas (arrows). Histological section (f) (H&E, 40×) reveals a mass composed of cells with clear cystoplasm, arranged in a nesting pattern, proven to be metastatic renal cell carcinoma by immunohistochemistry
Fig. 12.3
Pancreatic metastasis from renal cell carcinoma. An 81-year-old male with history of multiple cancers, including B-cell lymphoma in the cervical region 11 years prior, malignant melanoma in the back 34 years prior, and renal cell carcinoma that was treated 26 years earlier with left nephrectomy. A follow-up serial PET/CT scan (a) axial and (b) coronal images demonstrate a hypermetabolic area in the region of the head of the pancreas (arrows). CECT axial (c, d) and coronal (e, f) images demonstrate a heterogeneous mass in the head of the pancreas (arrows). Note the absence of dilatation of the pancreatic duct or bile duct associated with this mass. Intraoperative ultrasound gray scale (g, h), and color and power Dopper (i, j) transverse images show a hypoechoic, hypervascular mass involving the head of the pancreas (arrow). Patient underwent a Whipple procedure. Photographs of the resected specimen (k, l) show a round, golden-yellow mass with infiltrating borders (arrows) and hemorrhagic areas. Histological sections (m, n) revealed a vascularized tumor composed of polygonal cells with clear cytoplasm that have a tubular/acinar pattern, consistent with renal cell carcinoma, clear cell type. Morphologically identical to the primary renal cell carcinoma resected years before (H&E, 4×, 60×)
Fig. 12.4
Pancreatic metastasis from renal cell carcinoma. A 61-year-old female with neutropenia of unclear etiology. History of renal cell carcinoma that was treated 22 years earlier with left nephrectomy . MR shows two round lesions in the proximal pancreatic body with: (a) low signal intensity in fat-suppressed gradient echo T1-weighted image (arrows), (b) intermediate signal in T2-weighted image (arrows), and (c) homogenous enhancement (arrows) in contrast-enhanced fat suppressed gradient echo T1-weighted image. Note the absence of pancreatic duct dilatation associated with these lesions. Intraoperative ultrasound gray scale (d) shows two hypechoic, well-circumscribed masses in the body of the pancreas (arrows), and color Doppler (e) transverse scan of the larger lesion (arrow) shows a hypervascular mass. Patient underwent a distal pancreatectomy and splenectomy. Intraoperative photograph (f) shows a small mass with smooth borders in the body of the pancreas (arrows). Photograph of the bivalved larger mass (g) located in the body of the pancreas shows a well-circumscribed, yellow pancreatic mass with small hemorrhagic areas (arrows)
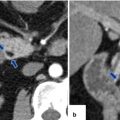
Fig. 12.5
Pancreatic metastasis from renal cell carcinoma. A 71-year-old male patient with past medical history of renal cell carcinoma that was treated 8 years earlier with left nephrectomy . Complaining of fullness in the epigastric region. CECT arterial phase axial image (a) shows a round well-circumscribed hypervascular mass in the body of the pancreas (arrow). In CECT portal phase axial (b) image, this mass becomes almost isodense with the rest of the pancreas (arrow). Intraoperative photograph (c) shows a pancreatic mass with smooth margins (arrow). Photograph of distal pancreatectomy and splenectomy (d) shows the pancreatic mass (arrows). Photograph of the bivalved specimen (e) shows a solid, soft, yellow mass abutting the splenic artery (arrow)
Fig. 12.6
Duodenal and pancreatic metastases from renal cell carcinoma. A 49-year-old male with history of renal cell carcinoma that was treated 9 years earlier with right nephrectomy. Patient complained of dizziness and was found to have upper GI bleeding. Upper endoscopy showed a fungating mass in the second portion of the duodenum. PET/CT axial image (a) demonstrates a hypermetabolic mass in the region of the head of the pancreas and duodenal region (arrows). CECT coronal (b, c) and axial (d) images show a large heterogeneous hypervascular mass involving the second portion of the duodenum as well the head of the pancreas. Patient underwent a Whipple procedure. Photograph of the gross specimen (e) shows a large irregular fungating mass with ulcerated and necrotic areas (arrow) protruding from the head of the pancreas into the second portion of the duodenum. Final pathology showed a metastatic renal cell carcinoma involving the second portion of the duodenum and the pancreatic head

Fig. 12.7
Diffuse pancreatic metastases from renal cell carcinoma. A 55-year-old female with history of a renal cell carcinoma that was treated 13 years earlier with right nephrectomy. CECT axial image shows diffuse heterogeneous enlargement of the body and tail of the pancreas (arrows). In addition, a necrotic metastatic deposit is noted in the right lobe of the liver (arrowhead) and small amount of free intraperitoneal fluid
Fig. 12.8
Pancreatic metastases from renal cell carcinoma. A 56-year-old female patient with history of renal cell carcinoma that was treated 6 years earlier with right nephrectomy . CECT axial arterial phase (a) and coronal portal phase (b) images demonstrate a well-circumscribed, hypervascular mass in the uncinate process of the pancreas (arrows). Note the absence of the right kidney. Patient underwent a Whipple procedure. Final pathology: metastatic renal cell carcinoma
Fig. 12.9
Simultaneous metastases in the pancreas and contralateral kidney. A 62-year-old male patient with history of left nephrectomy for renal cell carcinoma. Contrast-enhanced fat-suppressed gradient echo T1-weighted images (a, b) show a large heterogeneous, lobulated, hypervascular mass in the body of the pancreas as well as heterogeneous hypervascular mass in the right kidney (arrows). Note the absence of the left kidney
Fig. 12.10
Simultaneous metastases in the pancreas, adrenal gland, contralateral kidney, and bone from renal cell carcinoma. A 71-year-old female patient with history of renal cell carcinoma that was treated 28 years earlier with right nephrectomy . CECT axial images (a) show a hypervascular mass in the right adrenal (arrow), (b) a well-circumscribed, hypervascular mass in the head of the pancreas (arrow) and a heterogeneous mass in the left kidney (arrowheads), and (c) a large, destructive, expansile soft tissue mass involving the right iliac bone (arrow). Histological section (d) (H&E, 10×) shows a tumor composed predominantly of round to oval cells with abundant, clear cytoplasm and thin capillary network
Fig. 12.11




Metastatic melanoma to the pancreas. A 48-year-old male with history of melanoma arising in the right back, status post wide excision and axillary node dissection. A follow-up axial PET/CT image (a) performed 8 months after initial presentation, shows a hypermetabolic mass in the body of the pancreas (arrow). CECT axial image (b) show an ill-defined hypodense mass in the body of the pancreas (arrows). Note the extension of this mass inside the splenic vein (arrowhead). Patient underwent a distal pancreatectomy. Histological sections (c–f) (H&E, 40×, 100×) show the interphase between normal acinar cells and metastatic melanoma cells, that display a polyhedral shape with large nuclei and prominent nucleoli. Of note, several malignant cells contain melanin pigment (arrowheads). Tumor thrombus in the splenic vein was grossly observed
Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
