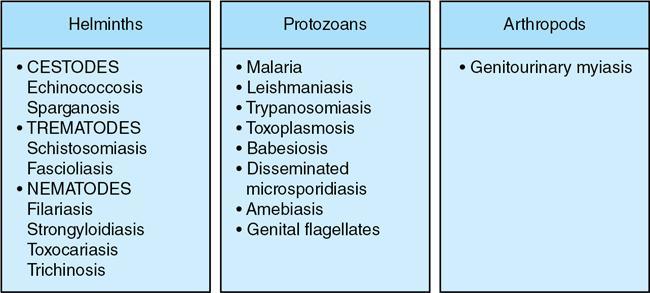
Parasitic infections of the genitourinary system are a group of diseases that have few common features.
Renal involvement is not among the common presenting features. While many parasites enter into the urinary tract, however only three parasitic infections are relatively common, that is schistosomiasis, echinococcosis and filariasis.
Schistosomiasis
Genitourinary schistosomiasis is caused by a fluke, Schistosoma haematobium. It is mostly seen in Africa and the Middle East. It can be seen in other countries due to travel or immigration.
Epidemiology
Schistosomiasis is common in tropical and subtropical regions.
Two forms of schistosomiasis exist: intestinal and genitourinary. Intestinal schistosomiasis can be caused by any of the species of blood flukes. However, genitourinary schistosomiasis is caused only by Schistosoma haematobium.
Children are affected, most commonly 5 to 15 years of age.
After their excretion by the mature parasite, the eggs migrate through the host’s bladder wall and are shed in urine or faeces.
Clinical manifestations
Clinical features correlate with the parasite’s developmental stage and the host’s response to the parasite and its eggs.
1. During the early stage of infection, the patient may present clinically with
• Dermatitis caused by cercarial penetration of the skin.
• Bronchopulmonary manifestations due to the passage of schistosomula through the lungs.
2. About 5 weeks after infection, Katayama disease may develop, which is characterized by marked clinical features such as malaise, weight loss, gastrointestinal symptoms, eosinophilia and fever.
3. The stage of egg deposition is manifested by symptoms of cystitis, dysuria with terminal haematuria, dull suprapubic pain and haemospermia.
4. Haematuria, the first clinical sign of genitourinary schistosomiasis, appears 10–12 weeks after infection.
Definitive diagnosis is based on identification of ova at microscopic analysis of urine specimens.
Imaging findings
Radiologic manifestations of urinary tract schistosomiasis are seen mainly in the ureters and bladder.
1. URETER
• Ureteral involvement in schistosomiasis has been reported in 65% of cases.
• The earliest change at cystography is persistent filling of the distal ureteral segment followed by distal ureteral dilatation. Early-stage ureteral dilatation results from ureteral dysfunction and not tissue damage which is generally unilateral.
• At a later stage, ureteral fibrosis may lead to ureteral strictures, most commonly in the intravesical segment of the ureter. The second most common location is 2–5 cm above the orifice.
• Fine ureteral calcification may be seen as a linear or parallel pattern on radiographs and as a circular pattern on axial CT images. These imaging findings are pathognomonic.
2. BLADDER
Due to submucosal oedema and pseudotubercles the bladder wall becomes hazy and ill defined. Later, it becomes thickened and ulcerated with multiple small papilloma that can be distinguished from a malignancy at cystoscopy and bladder biopsy.
Schistosomiasis is the most common cause of bladder wall calcification (Fig. 10.12.2.12.2). It is due to the presence of a large number of calcified dead eggs in the submucosa. The classic presentation of chronic urinary tract schistosomiasis is a calcified bladder, which resembles a foetal head in the pelvis.
• Calcifications may be coarser and thicker in empty bladder. Other patterns such as fine granular, fine linear and thick irregular calcification may be seen.
• Schistosomal Bladder Masses: chronic irritation of the bladder mucosa causes an inflammatory reaction. These buds then form into cystic deposits leading to cystitis cystica. At cystoscopy, the mucosa usually has a cobblestone-like appearance. In addition, in late stages, a papillary or polypoid mass may arise that mimics carcinoma and is commonly seen in the bladder neck and trigone.
• Squamous Cell Carcinoma: Schistosomiasis infection constitutes a major risk factor for bladder malignancies, predominantly for squamous cell carcinomas, which account for 50% of bladder cancers. Chronic infection causes squamous metaplasia, which may evolve into squamous cell carcinoma. A fungating mass is seen on radiologic images in about 80% of cases. The tumour may appear as a single enhancing mass or as diffuse or focal regions of bladder wall thickening.
The multiplicity of tumours is seen in 25% of cases.
• Chronic fibrosis and ureteral stenosis may result in vesicoureteral reflux as a late complication.
3. KIDNEY
• S. haematobium infection may cause a ureteral obstruction and vesicoureteral reflux. However, the renal disease develops slowly.
• MR urography is the imaging modality of choice for assessing the morphologic characteristics and function of the urinary tract.
4. GENITALS
• Calcification of the prostate gland, seminal vesicles or bladder wall seen on transrectal ultrasonography (US) or CT (Fig. 10.12.2.12.3) raises the suspicion of schistosomiasis.
• Chronic prostatitis is associated with seminal vesiculitis in the setting of schistosomiasis. On MRI, prostate may be normal in size with low signal intensity in the peripheral zone on T1- and T2-weighted images.
• Schistosomiasis of the testis is also known as bilharzial orchitis. Testicular oedema is common. In some patients, a testicular granuloma may simulate a mass.
• Fallopian tubes blockage and tubo-ovarian abscess formation may be seen.
• Vulval and perineal lesions may be hypertrophic, ulcerative, fistulous or wartlike.
Only gold members can continue reading. Log In or Register to continue