Chapter 16. Pediatric Studies
Patient Preparation
• Fasting time is not necessary or shorter for the pediatric age groups. No preparation for urinary examinations is required, but the bladder should not be emptied immediately before the examination. Pelvic sonograms in children should only require that the child not void immediately before the examination.
• Examining babies and small children requires that distractions are used to obtain cooperation during the examination. A parent should be in the room with the child. The examination should be explained to the parent or to the older child; demonstrate putting the transducer on your skin to show that the examination will not hurt.
• Neonates should be kept as warm as possible during the examination; warm gel should always be used, an external warming lamp may be used, and time spent scanning should be kept to a minimum. The neonate should be disturbed as little as possible.
• Neurosonograms require that the anterior fontanelle is accessible (intravenous needle must be removed).
Equipment and Technical Factors
• High-frequency transducers are commonly used for babies and small children. A linear array is used for pylorus and hip studies. A small footprint, high-frequency annular array, or sector transducer is used for neurosonograms of neonates; infants and older babies may require a lower-frequency transducer.
• Multiple focal zones may be used for a neurosonogram.
• Color Doppler imaging can be used to distinguish vascular from nonvascular structures and to identify vessels adjacent to the organ/structure of interest.
• Transducer covers should be used in cases of suspected infection.
Imaging Protocol
• Minimum documentation images for all examinations should include longitudinal and transverse axes images. Breathing techniques can be used for older children.
Minimum documentation images for the pylorus
• Longitudinal and transverse axes images with measurement of the length and wall thickness of the pylorus should be obtained. Images demonstrating fluid in the antrum of the stomach with or without passage of the fluid through the pylorus should be obtained. The patient may be placed supine or in a right oblique or decubitus position.
Minimum documentation images for the neurosonogram
• Specific positioning of the head is not as critical as is access to the anterior fontanelle. The anterior fontanelle coronal and modified coronal planes (C1–C7) are used to demonstrate the frontal lobes through the occipital lobes and the sagittal and parasagittal planes (ML-Sag 3–4) to demonstrate the midline structures through the far lateral aspect of the brain.
• Sagittal and parasagittal imaging should display the anterior portion of the brain toward the left of the screen and the posterior portion to the right. The coronal and modified coronal images, which display the right side of the brain, are on the left side of the screen.
• Other fontanelles may be used for imaging, if needed, but will not result in the above standard images.
Minimum documentation images for the dynamic infant hip examination
• Coronal and transverse images of the acetabulum and femoral head and neck with the hip in neutral position at rest and in flexion should be obtained. With hip flexion, the femur is abducted, adducted and stress maneuvers are done.
• Examination without abduction, adduction, and stress maneuvers may be done with the infant in a Pavlik harness.
Measurements
CBD
• <1.0 mm neonate
• <2.0 mm infant less than 2 years of age
• <4.0 mm child between 2 and 12 years of age
• <5.0 mm adolescent
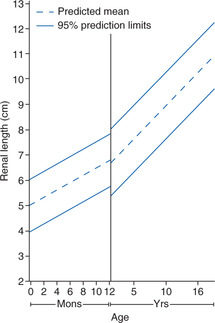
Kidneys
• Size varies with age. In older children, kidney size can also be related to the height and weight of the child if the kidneys are small or large for age.
Pylorus
• <3.5 mm wall thickness
• <17.0 mm in length
Uterus (Premenarchal)
• Length: 3.3–5.4 cm (cervix: 3.0 cm)
• Width: 0.7–1.6 cm
• Depth (AP): 0.7–1.6 cm
• Neonate: Uterine fundus larger than in a child because of maternal hormone stimulus
Ovarian volume
• 0.523 (L × W × D)
• Premenarchal: 3.0 cm3
Neurosonogram (neonate)
• Oblique diameter of ventricle body: <3.0 mm
• Width of third ventricle in coronal view: <2.0 mm
| Pediatric Studies | |||
|---|---|---|---|
| Sonographic Finding(s) | Clinical Presentation | Differential Diagnosis | Next Step |
Pyloric wall is thickened and pylorus is elongated Thickness of wall: >4.0 mm Length: >17.0 mm “Beaking” sign of fluid in antrum | Usually a first-born infant male, 4–6 weeks of age Projectile vomiting Failure to thrive (FTT) | Hypertrophic pyloric stenosis | Evaluate pylorus for spasm, passage of fluid |
In a newborn/infant/child, a kidney is absent in renal fossa, the ipsilateral adrenal is elongated, and renal arteries cannot be demonstrated with color Doppler imaging Ipsilateral ectopic kidney is not identified | Suspected anomaly from prenatal sonogram | Unilateral renal agenesis | Associated with reproductive system anomalies Contralateral kidney will be normal sized at birth but will demonstrate compensatory hypertrophy between 6–12 months of age |
| Kidney has a “lumpy” appearance | Asymptomatic | Fetal lobulation | Normal feature of kidney development in utero that may persist into adulthood |
| Triangular echogenic focus noted between the mid and upper sections of kidney | Asymptomatic | Junctional parenchymal defect | May also be seen with an interrenicular septum Remnant of fetal renal lobes |
Cortical tissue is noted between areas of echogenic renal pelvis Kidney may be normal or somewhat larger in size May be noted bilaterally | Asymptomatic | Bifid renal pelvis | Mildest form of kidney duplication Renal pelvis is singular at the renal hilum |
Duplication of renal collecting system with duplication of proximal ureters Ureters may rejoin distal to kidney and proximal to bladder Kidney is usually larger than normal May be noted bilaterally | Asymptomatic | Partial duplication Duplex collecting system | Reproductive anomalies may be present |
Duplication of renal collecting system and ureters Ureters enter bladder through separate orifices Hydronephrosis of the superior pole collecting system with/without hydroureter may be noted May be noted bilaterally | History of urinary tract infections | Complete duplication | Ureterocele may be noted as superior pole ureter inserts abnormally Echogenic dysplastic parenchyma may develop in upper pole of kidney |
Hydronephrosis in an infant or child Dilated calyces connect with dilated renal pelvis May be unilateral or bilateral | Abnormal prenatal sonogram Child: pain, hematuria, urinary tract infection, increased fluid intake | UPJ obstruction | Most common cause of hydronephrosis in children
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|
