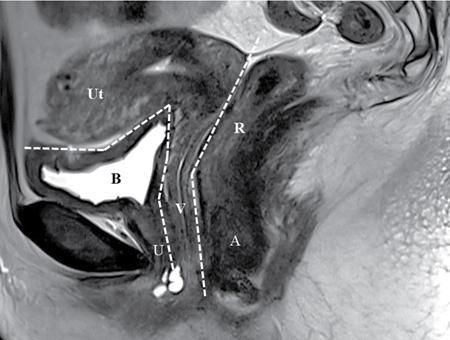
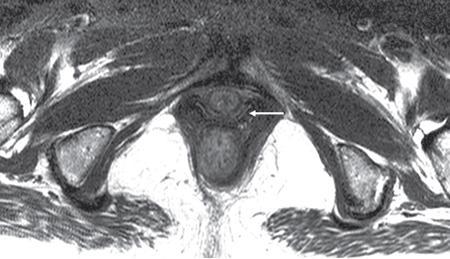
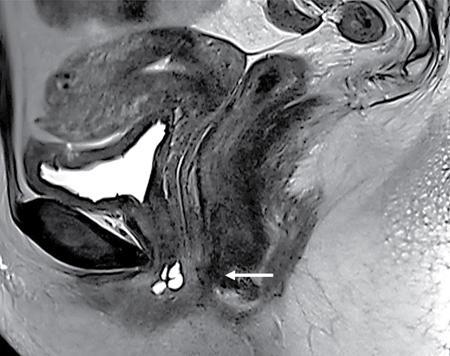
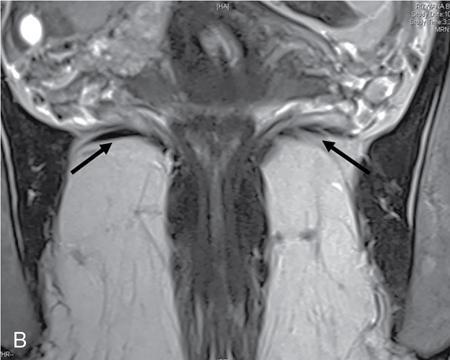
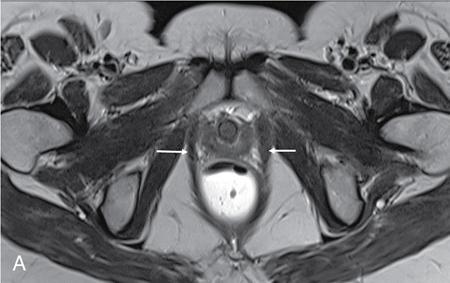
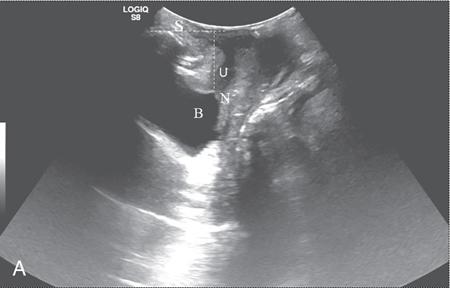
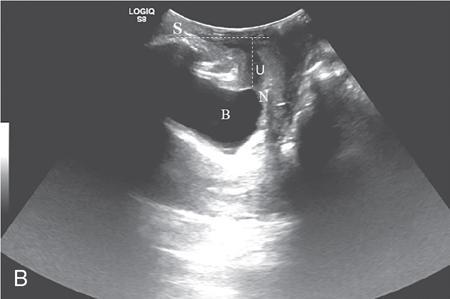
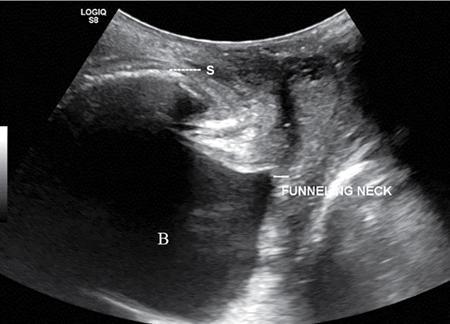
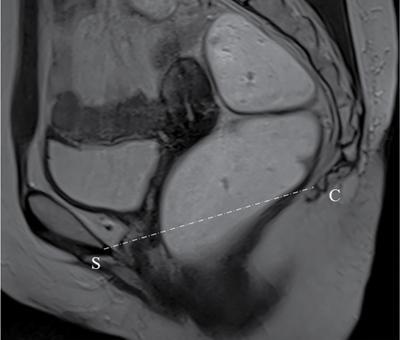
PELVIC FLOOR IMAGING – ANTERIOR AND MIDDLE COMPARTMENTS Anu Epean, Deepa Korula The term ‘Pelvic floor disorder’ refers to dysfunction of the pelvic floor musculature and connective tissues which provide support for the pelvic organs. This can produce a wide range of symptoms such a urinary incontinence, straining to void, dyspareunia, constipation, faecal incontinence and organ prolapse. The greatest risk factors for pelvic floor disorders are female sex and advanced age. Other risk factors include obesity, pregnancy, multiparity, smoking, connective tissue disorders. The pelvic floor is broadly divided into three compartments. The bladder and urethra form the anterior compartment. The vagina and uterus form the middle compartment and the posterior compartment comprises of the rectum and anal canal (Fig. 7.16.1.1). The attachment of the fascia, muscles and the ligaments to the bony pelvis form the support for these structures. From cranial to caudal, there are three layers which make up the pelvic floor – the endopelvic fascia, the pelvic diaphragm and urogenital diaphragm. This is the most cranial layer of pelvic floor, lying deep to peritoneum. It is a fine structure, comprising of a network of connective tissue which encases the pelvic viscera, provides support to the pelvic organs and maintains their anatomic relationship. There are several condensations of this fascia and ligaments which provide support in each of the pelvic compartments. In the anterior compartment, a fascial condensation called pubocervical fascia extends from anterior vaginal wall to the pubis. Tear in the pubocervical fascia can cause cystocele and urinary incontinence. There are three groups of ligaments which provide urethral support – periurethral, paraurethral and pubourethral ligaments. The periurethral ligaments arise from medial fibres of pubococcygeus and pass ventral to urethra. The paraurethral ligaments connect the lateral wall of urethra to periurethral ligament and pubourethral ligament connects the lateral wall of urethra to arcus tendineus. The urethra lies on a Hammock-like supportive layer of endopelvic fascia and anterior vaginal wall, which are stabilized by attachment laterally to arcus tendineus and levator ani (Fig. 7.16.1.2). In the middle compartment, condensations of the endopelvic fascia which attach the uterus to the lateral pelvic wall is called parametrium, which is made up of the uterosacral and cardinal ligaments. The uterosacral cardinal ligament complex supports and suspends the cervix and upper vagina above the levator plate. More inferiorly, the paracolpium attaches the vagina to the lateral pelvic wall. There are three levels of fascial support to the vagina: In the posterior compartment, the perineal body located within the rectovaginal septum supports ligaments and muscles and prevents abnormal widening of levator hiatus (Fig. 7.16.1.3). The rectovaginal fascia extends from posterior wall of vagina to anterior rectal wall. A tear in the rectovaginal fascia is the cause for an anterior rectocele. Arcus tendineus levator ani (ATLA) is formed by the condensation of the endopelvic fascia laterally, along the pelvic sidewall. This extends obliquely from inferior pubic symphysis to ischial spine and provides lateral support to the pelvic organs and attachment of the levator ani. Fascial condensations are not visualized on imaging; however, organ prolapse, due to deficiency in any of these, can be detected on MRI. The levator ani and the coccygeus muscles make up the pelvic diaphragm. The levator ani is the primary muscle of the pelvic diaphragm and is attached to the pubis and to the ATLA laterally on both sides. The slow twitch fibres of the levator ani continuously contract, maintaining tone to the pelvic floor and suspending the pelvic organs in the correct position. The two most important components of the levator ani are the iliococcygeus and puborectalis muscles. The iliococcygeus arises from external anal sphincter and has a curved shape, concave inferiorly. It fans out laterally to its insertion in the posterior part of arcus tendineus (Fig. 7.16.1.4A and B). Posteriorly, in the midline, condensations of ilococcygeus form a firm raphe anterior to coccyx called the anococcygeal ligament or levator plate. The pubococcygeus muscle is a component of the levator ani. It forms the anteromedial part and is a thick bundle of fibres arising from the pubis and anterior portion of arcus tendineus. It extends horizontally back to behind the rectum, medially forming the margin of urogenital hiatus (Fig. 7.16.1.5A). The anorectal and urogenital hiatus are closed by the contraction of the pubococcygeus muscle. This enables support during rest and in situations where the intraabdominal pressure is increased. The medial fibres of pubococcygeus, depending on their attachment to urethra, vagina, anus and rectum are termed as pubourethralis, pubovaginalis, puboanalis and puborectalis, collectively as pubovisceralis. The puborectalis forms a sling around the rectum (Fig. 7.16.1.5B). The muscles of the pelvic diaphragm are well delineated on MRI. The urogenital diaphragm or perineal membrane is the most caudal layer of the pelvic floor. It has a triangular appearance, extending from the pubic symphysis and the ischiopubic ramus to the posterior perineal body. It is ventral to the external anal sphincter and perineal body. It is attached to the surrounding structures such as the perineal body, external anal sphincter, vagina and the bulbocavernosus muscle. Imaging has an increasing role in the evaluation of pelvic floor disorders. Clinical examination alone has a low sensitivity and specificity for the detection of multicompartment involvement and organ prolapse. Imaging helps to detect involvement of multiple pelvic compartments and thus to plan surgery. Ultrasound, MRI and conventional imaging which includes voiding cystourethrography, evacuation proctography and dynamic cystocolpoproctography (DCP) are used to evaluate the pelvic floor. It is easily available, cheap and does not involve ionizing radiation. In the evaluation of the anterior compartment, ultrasound is more reliable than MRI. Transperineal ultrasound using 2D, 3D or 4D techniques along with dynamic imaging helps to evaluate pelvic floor dysfunction. Patient is placed in a dorsal lithotomy position for a transperineal scan although a standing position can also be used. Convex transducer (2–6 MHz) or endoluminal transducers (endovaginal/endorectal) maybe used. In a midsagittal translabial scan, the anatomic relationship of urethra, bladder, vagina, cervix and anorectum can be studied and the relative position of these organs determined by use of certain measurements. The bladder-symphysis distance (BND) is the distance between the bladder neck and lowest margin of symphysis pubis and demarcates position of the bladder neck. Measurement of BND is made at rest and during Valsalva manoeuvre and the difference in BND between the two, gives the measure of bladder neck descent. There are no definite values to indicate normal descent but there is a proposed cut off of 20, 25, 30 mm to indicate hypermobility (Fig. 7.16.1.6A and B). The proximal urethra rotates posteroinferiorly during Valsalva manoeuvre and this can be measured by the posterior urethrovesical angle (β) or the gamma angle. The posterior urethrovesical or retrovesical angle (β) is the angle between a line through the urethral axis and the line through the trigonal surface of the bladder and varies from 90–120 degrees normally. This may increase to 160–180 degrees and can be associated with funnelling of bladder neck. The gamma angle is the angle between a line through the inferior margin of pubic symphysis and the urethrovesical junction. This is seen on Valsalva manoeuvre or at rest in patients with stress incontinence (Fig. 7.16.1.7). Color Doppler can demonstrate urine leakage on performance of Valsalva or at rest. Other abnormalities that can be detected on transperineal ultrasound are cystocele, urethral diverticulum, Gartner duct cyst, foreign body or bladder tumour. 3D pelvic ultrasound is useful to evaluate pelvic floor dysfunction and to study the urethra, levator ani complex, paravaginal supports, prolapse and implant imaging. 4D ultrasound helps in real-time, dynamic imaging of pelvic floor. In the middle compartment, although uterine prolapse is often clinically evident, it can also be detected by ultrasound. Uterine prolapse can be also quantified by measuring maximum descent of uterus from the reference point which is the inferior margin of pubic symphysis. Ultrasound is also useful to evaluate for surgical planning in a large retroverted uterus with an anteriorly placed cervix causing voiding symptoms. MRI is useful in the evaluation of pelvic floor as it provides good anatomic detail about the pelvic floor muscles, ligaments because of its inherent superior soft tissue resolution. In addition, dynamic MRI yields functional information. MRI defecography is a dynamic study performed to study the posterior pelvic compartment but it also gives information about the anterior and middle compartments. It can be performed both with closed magnet and open magnet systems. The patient is positioned supine with phased array coil around pelvis in a closed magnet system. In an open magnet system, the patient is in a sitting and more physiological position; however, due to the lower signal to noise ratio and lower resolution, a closed magnet system is preferred. Bowel preparation with use of laxative on night before the scan is optional. Voiding prior to the study is encouraged since an overdistended bladder can cause misinterpretation of results. Presence of some urine in the bladder is however, helpful to detect anterior vaginal prolapse. Instructions are given to the patient, prior to the procedure, about the ‘rest’, ‘squeeze’, ‘strain’ and ‘defecate’ phases of dynamic imaging, to ensure that movement or lifting of the pelvis does not occur during these manoeuvres. The rectum is filled with up to 200 mL of ultrasound gel. The patient is made to wear an adult diaper and covered with an incontinence pad on the gantry. Vaginal gel, ∼50 mL maybe introduced since this helps to delineate anatomic landmarks and detect uterovaginal prolapse. Initial large FOV T1 localizer scans help to identify the midline sagittal section of pelvis. T2-weighted fast spin echo, high-resolution sequences in sagittal, axial, coronal planes are used to obtain anatomic detail. This is followed by dynamic imaging of the pelvic floor with use of steady state imaging sequences such as True fast imaging with steady state precession (TrueFISP Siemens) and balanced fast field echo (balanced FFE Philips). Steady state sequences have the advantage of short acquisition times and higher signal to noise ratio and hence useful to obtain rapid serial midsagittal images while patient performs ‘squeeze’, ‘strain’ and ‘defecates’. There are several points and lines for measuring and staging pelvic organ prolapse on MRI; however, the PCL line is said to have the highest interobserver and intraobserver reliability of MRI measurements compared to all proposed reference lines and is described below: Pubococcygeal line (PCL): defined as the line that connects the inferior portion of the pubic symphysis to the last coccygeal joint. The PCL is the most commonly used reference line for the assessment of pelvic floor disorders (Fig. 7.16.1.8).
7.16: Pelvic floor imaging
Introduction
Anatomy of pelvic floor
Endopelvic fascia
Pubocervical fascia
Urethral supports
Parametrium
Paracolpium
Delancey’s levels of vaginal support
Perineal body and rectovaginal fascia
Pelvic diaphragm
Levator ani
Iliococcygeus

Pubococcygeus

Urogenital diaphragm
Imaging
Ultrasound
Anterior compartment
Bladder-symphysis distance
Urethral hypermobility
Funnelling of bladder neck
Middle compartment
MRI
Technique
Protocol for MRI
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


