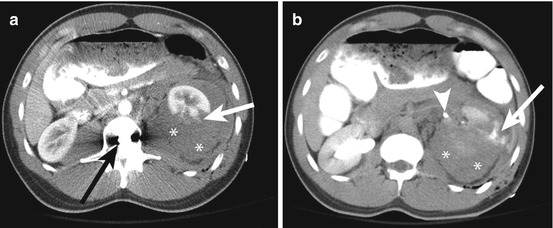
Fig. 36.1
A 23 year-old male presents with pain after sustaining a gunshot wound to the upper abdomen. (a) Post contrast computed tomography (CT) shows the tract of the bullet; the bullet entered the subcutaneous tissues in the left upper quadrant (arrow) and traveled tangentially to the right upper quadrant (arrowhead) without traversing the fascial layer. (b) Immediately inferiorly, the bullet (arrowhead) is lodged in the subcutaneous tissues of the right upper quadrant
The presence of extraluminal gas can be confusing, as it may be introduced at the time of assault or may be due to a bowel injury. Since a focal disruption in the bowel wall is rarely seen on CT, these patients may benefit from repeat imaging after ingestion of a water-soluble oral contrast agent if no laparotomy or laparoscopy is undertaken.
Posterior Injuries
CT provides an efficient, global view of the abdomen. The field of view should be chosen to include the entirety of the peritoneum, retroperitoneum, bony structures, adjacent soft tissues and skin surface. Inclusion of the skin surface is important as it may provide the first clue in identifying the site of injury. Generally, a focal site of skin disruption or subcutaneous gas indicates the entrance site of the penetrating object. After identifying this, the adjacent soft tissues and retroperitoneum in the trajectory of the penetrating injury need to be evaluated. Surgical exploration can usually be avoided in patients with penetrating wounds confined to the superficial tissues or sparing the retroperitoneal viscera, only causing a small hematoma (Fig. 36.2a, b). The triage of the patient largely depends on a CT performed according to proper protocol.
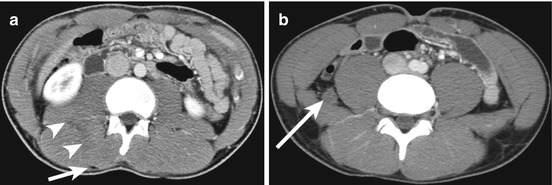
Fig. 36.2
A 20 year-old male sustained a stab wound to the right flank during assault. (a) Contrast-enhanced CT shows the stab wound entry site (arrow) and the tract (arrowheads) through the posterior musculature. (b) More inferiorly, there is a small hematoma (arrow) between the psoas and quadratus lumborum muscles. The retroperitoneal viscera were intact
Unless contraindicated, the CT should be IV contrast medium enhanced. While a non-contrast CT can identify the site of penetrating injury, provide a rough estimate of its depth, and detect a retroperitoneal hematoma, the lack of contrast medium renders the examination suboptimal. Particularly, the depth of a penetrating injury and the number and depth of renal lacerations may be severely underestimated. More importantly active hemorrhage and pseudoaneurysms cannot be diagnosed. Determination of active hemorrhage is a critical finding, as either angio-embolization or surgical intervention is usually indicated. Additionally, the use of intravenous contrast medium may allow characterization of the retroperitoneal fluid. In the presence of peri-nephric fluid or suspected hematoma the acquisition of delayed phase imaging during the excretory phase is crucial for accurate assessment of retroperitoneal injury. Extravasation of contrast during the excretory phase indicates disruption of the renal collecting system, renal pelvis or ureter. When correlated to coronal reformatted images, the site of the leak can often be identified, which helps with interventional planning (Fig. 36.3a, b).