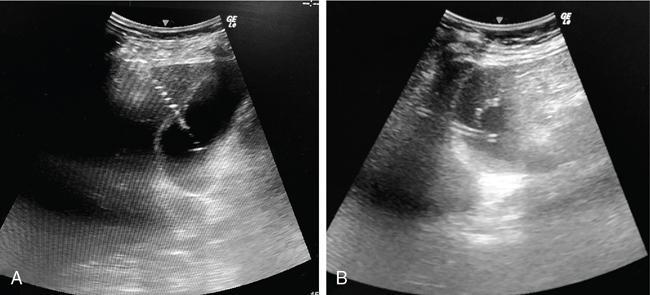
PC is a minimally invasive procedure which involves placement of a drainage catheter into the gallbladder, usually under USG guidance. It is most commonly performed to decompress an inflamed gallbladder in cases where surgery is not possible due to associated comorbidities. The indications of PC can be divided into those that require access into the gallbladder and those that require biliary tract access. The common indication for PC is acute cholecystitis due to calculus obstruction of the gallbladder neck or cystic duct in poor surgical candidates or patients with severe cholangitis. The definitive treatment for acute cholecystitis is laparoscopic cholecystectomy. Another application is for stone removal or percutaneous cholecystolithotomy through this route. PC can also be used for biliary drainage or decompression in cases where the biliary system is not dilated, particularly when the obstruction is below the level of cystic duct–bile duct junction. PC is also used for biliary diversion in the setting of a bile leak or duodenal fistula in inflammatory or traumatic conditions, thereby reducing the risk of biliary peritonitis. For intraluminal procedures, PC can act as an access portal in case the peripheral bile ducts are inaccessible. The prerequisite for PC is that the gallbladder must be distended for allowing its puncture. Contraindications to PC include unavoidable interposed bowel segment between the gallbladder and the puncture site and biliary peritonitis. Presence of coagulation disorders is a relative contraindication. This includes review of the patient’s clinical status and imaging. Screening USG should be done to evaluate the gallbladder – whether distended or not, the site of obstruction, and to decide the approach. PC is usually performed under real-time USG guidance. CT or fluoroscopic guidance is rarely used due to limited availability, exposure to ionizing radiation and higher cost. In sick patients, the procedure might need to be performed at the bedside, making USG a suitable modality. Like other invasive procedures, the blood parameters need to be evaluated (PT/INR, platelet count, renal function tests). An informed consent should be obtained. Intravenous access should be established. Patients who are candidates for cholecystostomy are usually sick and are usually on antibiotic treatment. In case where it is not so and there is clinical evidence of infection, third-generation cephalosporins and macrolides for covering anaerobic bacteria may be administered. This procedure is mostly done under USG guidance as this technique is readily available for bedside and emergency procedures and more cost-effective. It can also be performed under CT or fluoroscopy guidance. The procedure is done under local anaesthesia. The patient lies supine or in the left lateral position and the area is cleaned and draped. Based on the position of the gallbladder, a preferable access route is chosen, either transhepatic or transperitoneal. The second decision is about the puncture technique, which may be modified Seldinger or trocar. An 8F catheter is usually placed to allow drainage of bile. If the bile is thick and infected, a 10F or 12F catheter may be necessary. Locking pigtail catheters are useful in reducing the incidence of catheter dislodgement. The two USG-guided approaches used for PC are transhepatic and transperitoneal, of which the former is usually preferred. In the transhepatic approach (Fig. 9.24.14), the gallbladder is punctured through the liver parenchyma, generally the bare area. The traversed liver parenchyma provides better support for the catheter and helps in reducing the incidence of bile leak into the peritoneal cavity and thus biliary peritonitis. However, since liver is a vascular organ, there is an increased risk of bleeding due to the puncture of the liver. Thus, this approach should be cautiously used in patients with liver dysfunction and coagulopathies.
3. Percutaneous cholecystostomy
Indications/contraindications
Preprocedure evaluation
Patient preparation
Procedure details
Transhepatic versus transperitoneal approach
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


