Percutaneous Discectomy
Lubdha M. Shah, MD
Key Facts
Terminology
Percutaneous disc removal to reduce intradiscal pressure → protruded disc retracts back in place, reduced irritation on annulus nociceptive nerve receptors
Also decompresses nerve root from disc
Another proposed mechanism is that removing disc material may prevent release of chemical mediators that directly injure nerve root
Pre-Procedure
Radicular pain usually greater than back pain/neck pain
Positive CT or MR scan for disc herniation
Contained herniated disc of < 6 mm
Contained herniated discs have intact outer annulus with displaced disc material held within outer annulus of contained herniated disc
Noncontained herniated disc has localized displacement of disc material beyond intervertebral disc space & breach in outer annulus
No improvement of symptoms after 6-8 weeks of conservative therapy
Before PD, pain relief should be confirmed after selective nerve root block has been performed
Post-Procedure
PD may provide appropriate relief in properly selected patients with contained lumbar disc prolapse
Reduced procedure time, lower costs, quick recovery, and low complication rates that can include discitis and possible nerve injury
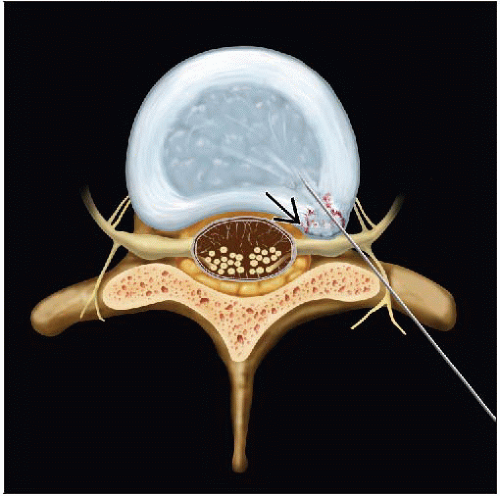 PD reaches the disc via a posterolateral approach, passing just anterior to the superior articular facet, behind the nerve, in a trajectory toward the center of the disc. A contained foraminal protrusion is noted  . . |
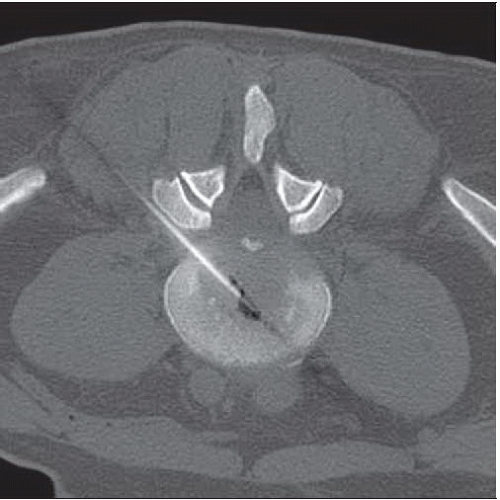 Axial NECT shows automated probe passing anterolaterally to the herniation and coming to rest in the center of the disc. Most of the disc removal occurs 1 cm anterior to the herniation. |
TERMINOLOGY
Abbreviations
Percutaneous discectomy (PD)
Synonyms
Automated PD
Definitions
Percutaneous disc removal reduces intradiscal pressure
Protruded disc retracts back, which helps reduce irritation on annulus nociceptive nerve receptors
Also decompresses nerve root from disc
Another proposed mechanism is that removing disc material may prevent release of chemical mediators that directly injure nerve root
PRE-PROCEDURE
Indications
Radicular pain usually greater than back pain/neck pain
Symptoms include sensory loss, tingling, numbness, & muscle weakness
Positive CT or MR scan for disc herniation
Contained herniated disc of < 6 mm
Contained herniated discs have intact outer annulus with displaced disc material held within outer annulus of contained herniated disc
Noncontained herniated disc has localized displacement of disc material beyond intervertebral disc space & breach in outer annulus
No improvement of symptoms after 6-8 weeks of conservative therapy
Positive electromyogram study is helpful
Contraindications
Evidence of acute or progressive degenerative spinal cord diseases
Evidence of neurologic or vascular pathologies mimicking herniated disc
Evidence of advanced spondylosis (significant bony spurs) with disc space narrowing, diffuse annular bulging, or spondylolisthesis
Evidence of significant bony spurs blocking entry to disc space
Evidence of cervical spinal canal or lateral recess narrowing
> 50% compromise of spinal canal by herniated disc
Evidence of large extruded disc or sequestered disc fragment
Existence of other pathologies or conditions, such as fractures, tumors, pregnancy, or active infections
Previous surgery at site of herniated disc
Getting Started
Things to check
Coagulation parameters
Complete blood count, platelet
Allergies
Medications
Lidocaine
Minimal sedation with midazolam and fentanyl to reduce anxiety and help control blood pressurerelated changes
Equipment list
18-gauge hubless sheath with central trocar is guided toward affected disc
Trocar is removed, and smaller 2.5 mm cannula with inner blunt end sleeve is placed over hubless sheath
Once correct placement is confirmed, hubless sheath is removed, leaving 2.5 mm cannula
2 mm saw is threaded through cannula, and hole is cut into annulus for aspiration probe to be inserted
Aspiration probe is sharpened cannula fitted through outer needle
Using suction to pull in disc material, the inner, sharpened cannula uses slide-like cutting motion to slice tissue
Tissue is then aspirated, along with irrigation, through inner cannula to collection bottleRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree