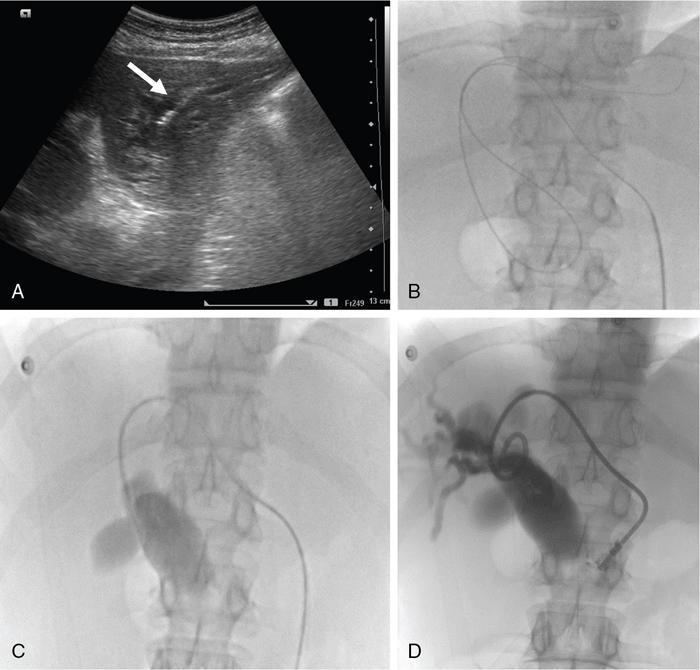
The relief of obstructive jaundice following the placement of a percutaneous transhepatic catheter was first described by Dr William Molnar and Dr Alfred Stockum in 1974. This technique involves aseptic percutaneous puncture of a peripheral biliary radicle, followed by fluoroscopy-guided wire and catheter manipulation and insertion a drainage catheter (pigtail or ring biliary catheter) or stent for drainage. PTBD is performed as a therapeutic and as a palliative procedure. The indications for PTBD can be divided into malignant and benign causes (Table 9.24.1). The aims of PTBD in these indications are shown in Table 9.24.2. For malignant aetiologies, PTBD is useful in preoperative and palliative settings, and for benign aetiologies it may be a bridging procedure before a definitive surgery or therapeutic. Hyperbilirubinemia limits the selection of chemotherapeutic agents. Chemotherapeutic agents such as anthracyclines (doxorubicin), topoisomerase inhibitors (irinotecan) and the taxanes require intact mechanisms of bilirubin excretion to prevent toxicity. Bilirubin level less than 2–3 mg/dL is usually considered safe for most of these agents. In addition, preoperative biliary drainage helps in the reduction of renal toxicity caused by bilirubin and thus reduces surgical morbidity. Altered enterohepatic circulation due to biliary obstruction leads to symptoms such as anorexia and altered food taste and these symptoms are relieved with biliary drainage. Pruritus is another such symptom which hampers quality of life. Drainage of even one liver segment causes significant relief in pruritus. Various intrabiliary procedures such as brush biopsy, brachytherapy and RFA (explained later in the chapter) can be done through the same route. Benign biliary strictures (BBSs) usually require percutaneous approach as endoscopy is either difficult, such as in postoperative bilioenteric anastomotic strictures or has failed, as in tight distal strictures precluding bile duct or ampullary cannulation. Biliary diversion through PTBD is important in cases of posttraumatic bile leak to prevent peritonitis and sepsis. Uncommonly, in cases where the benign bile duct strictures extend to the hepatic hilum and intrahepatic parts of distal segmental ducts, it may be difficult for the surgeon to locate the duct intraoperatively. In such situations, percutaneous placement of a catheter preoperatively facilitates duct identification at surgery. There are no absolute contraindications. Relative contraindications are coagulation disorders, allergy to iodinated contrast agents and ascites. In cases with abnormal coagulation profile requiring emergency biliary drainage (patients in cholangitis with risk of septicaemia), fresh frozen plasma should be given before and during the procedure. In elective cases, vitamin K injection may be given for 3 days and procedure should be done after normalization of coagulation parameters. In rare emergent scenarios where coagulation profile of the patient is not known, drainage can be done immediately. However fresh frozen plasma should be kept ready. Large-volume ascites causes technical difficulty and predisposes to peritonitis and bleeding. Thus, ascites must be drained prior to PTBD. In cases of allergy to a particular iodinated contrast agent, a different category of contrast agent may be used. Before performing the procedure, the following aspects must be evaluated. Reviewing baseline imaging is the most vital step required to perform a successful biliary intervention. All patients requiring a percutaneous biliary intervention should have had a multiphase contrast-enhanced cross-sectional imaging, either computed tomography (CT) scan or magnetic resonance imaging (MRI) before the procedure. Both modalities are equally accurate in assessing the cause and level of obstruction and outlining the extent of the disease. CT and MRI also provide an assessment of the volume of hepatic parenchyma. MRCP provides information about the extent of biliary dilatation, level of obstruction and presence of any variations in biliary anatomy. Bile duct obstructions can be high or low, above or below the level of cystic duct insertion, and identifying this is important. Distal obstructions are usually managed endoscopically, and percutaneous interventions are required when endoscopic drainage is unsuccessful, is contraindicated or when it is not technically possible. For high obstructions, percutaneous approach is easier and more targeted and thus preferred. A multidisciplinary team is involved in the final management decision which is tailored to each patient. Ultrasonography (USG) plays a considerable role during PTBD. It assists in screening the patient prior to any percutaneous radiological procedure, where it helps in the assessment of the extent of dilatation of the bile ducts, status of the primary and secondary confluences (patent or blocked), volume of the liver segments or lobes being drained, and presence or absence of ascites. Knowledge of these helps to decide the approach used, lobe to be drained and the hardware needed. A review of patient’s blood parameters is also required. The most relevant parameters are prothrombin time (PT) and international normalized ratio (INR). The PT values should not be more than 4 seconds above the control value and INR be below 1.5. The platelet count should be more than 50,000/μL. Renal function tests (blood urea nitrogen and serum creatinine) also need to be reviewed before the procedure, although it does not usually alter the management. The patient should be admitted in the hospital prior to the procedure. In elective cases, at least 3 hours of fasting for solids is required. An informed consent is required with mention of the catheter care required postprocedure. Intravenous access should be secured. Antihypertensive medications should not be skipped; oral hypoglycaemic agents and insulin should be avoided in view of fasting. Biliary drainage has been classified as clean-contaminated or contaminated according to the Society of Interventional Radiology and thus requires antibiotic prophylaxis. A dose of intravenous antibiotics (preferably third-generation cephalosporins and metronidazole to cover anaerobic bacteria) should be given 1 hour prior to the procedure, as transient bacteremia commonly occurs during PTBD. If more than 2 hours lapse from the initial dose, the dose may be repeated. Patients should be hydrated with 0.5–1 L normal saline prior to the procedure. Fluids can be chosen based on requirement. The procedure is usually performed under local anaesthesia (2% lignocaine) and light conscious sedation (midazolam or fentanyl may be used). Screening USG is repeated to replan the approach and to rule out ascites. All the hardware required should be kept ready (Figs. 9.24.1 and 9.24.2). The procedure is performed with the patient in supine position. The skin area, depending on whether the right or left or both ductal system needs drainage, is cleaned and draped. Local anaesthesia (2% lignocaine) is injected along the planned tract, up to the liver capsule. Then, a small nick is given on the skin using a surgical blade. The sectoral bile duct (usually segment 3 for left- and segment 6 for right-sided PTBD) is punctured peripherally using an 18G Chiba needle, under USG guidance (Fig. 9.24.3). Central duct punctures are more prone to vascular injuries and may also provide inadequate drainage of hepatic lobes.
1. Percutaneous transhepatic biliary drainage
Indications
Malignant aetiology
Benign aetiology
Contraindications
Preprocedure evaluation
Patient preparation
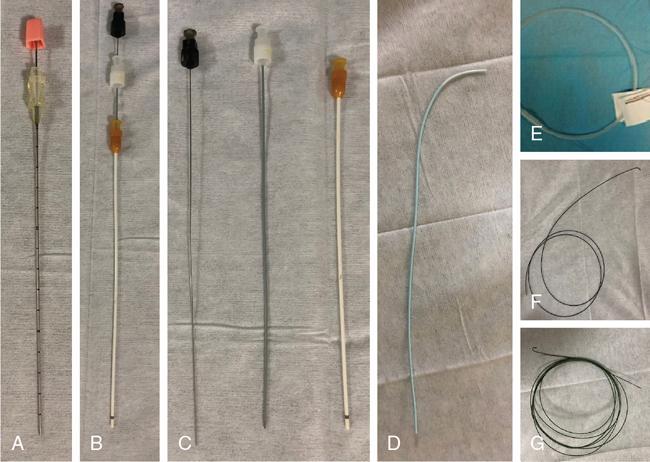

Procedure details
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


