PET/CT Artifacts
Todd M. Blodgett, MD
Ashok Muthukrishnan, MD
PET/CT Artifacts
AC Artifacts
Most common AC artifacts secondary to
Intravenous contrast
Oral contrast
Chemotherapy ports
Orthopedic devices
Dental implants/fillings
Calcified structures (lymph nodes)
Pacemakers
Methylmethacrylate (vertebroplasty)
Always check the non-AC images when there is apparent FDG activity associated with high HU
AC artifacts may be clinically relevant if misinterpreted as true pathology
Newer scanners have improved AC algorithms, and fewer artifacts are observed
Respiratory Artifacts
Most common: “Mushroom” artifact at or near the diaphragm
Consider using either a modified breath hold or performing a second CT with a breath hold
Other Issues that Negatively Affect Image Quality
Elevated blood glucose
Large patient body habitus
Infiltrated FDG dose
Beam hardening artifact when arms are down
CT Protocols
Multiple ways to perform the CT portion of a PET/CT to optimize protocols for various malignancies
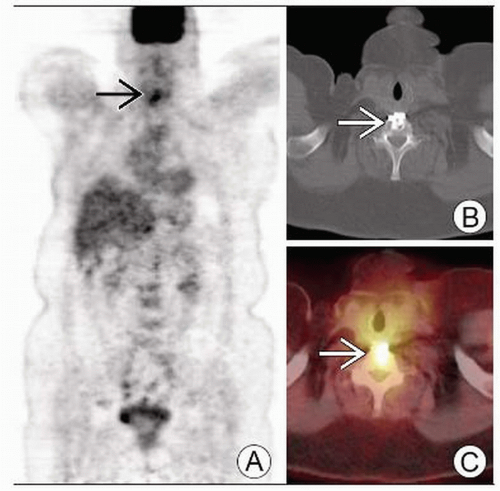 Coronal PET (A) shows a focal area of apparent increased FDG activity  correlating with an anterior fusion high attenuation orthopedic device correlating with an anterior fusion high attenuation orthopedic device  on axial CT (B) and fused PET/CT (C). on axial CT (B) and fused PET/CT (C). |
 Axial attenuation-corrected PET image (bottom) reveals apparent uptake  , which is not visualized on the uncorrected image (top) , which is not visualized on the uncorrected image (top)  . . |
TERMINOLOGY
Abbreviations
Attenuation correction (AC) artifacts, respiratory artifacts, beam hardening artifacts
Definitions
Artifacts encountered on PET/CT images
PATHOLOGY-BASED IMAGING ISSUES
Key Concepts or Questions
AC artifacts
Result from presence of IV and oral contrast on the CT used for AC correction
Advantage of PET/CT is ability to use CT for attenuation correction
Obviates the need for an extra transmission scan as performed on dedicated PET scanners
Use of CT for AC permits 40% reduction in examination time
AC algorithms tend to overcorrect objects with high attenuation, such as contrast agents and chemotherapy ports
Many artifacts are easily identified as such
Some presentations with atypical appearances can lead to more challenging interpretation
e.g., calcified lymph nodes
High attenuation material
Using older scanners may result in artifacts that mimic intense FDG uptake
May be clinically significant when located adjacent to true lesion
May occasionally appear as focal finding and mimic a malignant lymph node
True malignant lesion may be obscured by a contrast artifact
Newer scanners with better AC algorithms have lower incidence of AC artifacts
Methods for avoiding misinterpretation of AC artifacts
Simplest solution is to inspect the uncorrected PET images
When a scan is positive, check the uncorrected images
Can be cumbersome to switch between attenuation-corrected and uncorrected images on some viewing systems
Some fusion systems will not allow side-by-side comparison
Low dose CT prior to diagnostic PET/CT
Noncontrast CT can be performed prior to diagnostic PET/CT imaging to be used for AC
Disadvantages include additional radiation exposure, costs
Software solution
Most appealing means of handling AC artifacts
Methods are currently being investigated
Most vendors have upgraded AC algorithms installed in newer scanners
Imaging Approaches
Oral and IV contrast issues
Barium- and iodine-based oral contrast agents are highly attenuating on CT and tend to cause AC artifact
Water-based oral contrast agents generally do not cause artifact
Overlap of physiologic and artifactual bowel activity is common
Linear appearance of bowel activity on PET generally has limited clinical importance
Focal or irregular appearance should prompt inspection of uncorrected PET image
Clinical importance of these artifacts is unclear
Study results are conflicting
Software solutions being developed may simplify interpretation
Clinical importance of oral contrast
Ports and other high contrast materials
Metallic objects, including orthopedic devices and chemotherapy ports
May demonstrate falsely elevated FDG uptake on AC PET images (with CT-based attenuation correction)
Small malignant lymph nodes or soft tissue lesions adjacent to such devices can be more difficult to detect
Patient movement between PET and CT portions of exam can produce artifactual uptake in area of orthopedic devices
Uptake in this pattern may be mistaken for infection or loosening
Dental implants and fillings can produce artifactual uptake on PET
May obscure or mimic true lesions
Particularly pertinent in patients with head and neck malignancies
Metallic devices
Produce a photopenic area on dedicated PET
Produce increased apparent FDG activity on most PET/CT scanners
Newer scanners with improved AC algorithms may not cause artifacts
Calcified lymph nodes
Perhaps the most clinically significant AC artifact
Lung cancer patients can be erroneously upstaged by the presence of a single contralateral node
May lead to non-surgical management if artifact is not suspected
High index of suspicion must be used when calcified lymph nodes are seen on CT portion of exam
Focal apparent FDG uptake is particularly easy to misinterpret
Non-AC artifacts: Diaphragmatic motion artifacts
Diaphragm motion during CT scan can cause large portions of the liver to appear displaced into the thorax
Typically due to protocol that includes deep inspiration for CT acquisition and tidal-breathing for PET acquisition
Modified breathing algorithms can be used, such as breath-hold at normal end-expiration for scanning through liver
Lesions in superior liver or lower thorax are most likely to be misinterpreted secondary to these artifacts
Lesions may be located to the wrong organ
Radiotherapy applications hinge on accurate localization
Other image quality considerations
Lymphangiogram effect
FDG injection may accidentally be infused into subcutaneous tissue, leading to uptake into lymphatic system
Axillary or mediastinal lymph nodes may subsequently demonstrate intense FDG uptake
Study becomes non-diagnostic, and short term follow-up is recommended
Patient size
Photon attenuation is minimized with smaller body size
Results in images with good signal-to-noise ratio
Images quality generally degrades with increasing patient bulk
Consider slightly longer PET scanning times or increased FDG dose
Arm positioning
Arms in the imaging plane can cause significant beam-hardening and streak artifact in CT images
Positioning arms above thorax can lead to discomfort and motion artifact
However, scanning with arms up significantly improves image quality and should be performed when possible
Head and neck imaging can be performed separately with arms down
Blood glucose and insulin
Glucose competes with FDG for cellular entry, so elevated blood glucose can diminish image quality
Unfortunately, insulin promotes diffuse FDG uptake that can also impair diagnostic value of PET scan
Fat and muscle are affected, leading to diffuse linear FDG uptake in skeletal muscle
In general, good-quality PET/CT images depend on tight glucose control prior to scanning
Imaging Protocols
CT-based attenuation correction
Measured Hounsfield units (HU) must be transformed into corresponding quantity at higher PET photon energy of 511 keV
Most algorithms segment image pixels into soft tissue or bone, based on HU, and transform using scale factors
Other algorithms treat image pixels as mixture of two well-defined materials and transform them accordingly
CT portion of PET/CT examination
Three approaches to this portion of the exam
Low current CT (˜ 40 mAs): Used primarily for AC and localization
Normal current CT (˜ 140 mAs): With or without IV/oral contrast to provide diagnostic-quality image
Both low and normal current CT: Noncontrast low dose scan used for AC, and normal scan used for diagnostic quality imaging
CLINICAL IMPLICATIONS
Clinical Importance
AC artifacts may be clinically relevant when they have atypical appearances or are misinterpreted as pathology
RELATED REFERENCES
1. Hamill JJ et al: Respiratory-gated CT as a tool for the simulation of breathing artifacts in PET and PET/CT. Med Phys. 35(2):576-85, 2008
2. Nahmias C et al: Does Reducing CT Artifacts from Dental Implants Influence the PET Interpretation in PET/CT Studies of Oral Cancer and Head and Neck Cancer? J Nucl Med. 49(7):1047-1052, 2008
3. Bacharach SL: PET/CT attenuation correction: breathing lessons. J Nucl Med. 48(5):677-9, 2007
4. Chi PC et al: Design of respiration averaged CT for attenuation correction of the PET data from PET/CT. Med Phys. 34(6):2039-47, 2007
5. Cook GJ: Pitfalls in PET/CT interpretation. Q J Nucl Med Mol Imaging. 51(3):235-43, 2007
6. Kaneta T et al: High-density materials do not always induce artifacts on PET/CT: what is responsible for the difference? Nucl Med Commun. 28(6):495-9, 2007
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


