PETROUS APEX CHOLESTEROL GRANULOMA/CHOLESTEROLOSIS, MUCOCELE, AND EPIDERMOID CYST
KEY POINTS
- Magnetic resonance imaging can make the definitive diagnosis of cholesterolosis and mucocele of the petrous apex, especially when combined with typical computed tomography findings.
- Computed tomography is useful in treatment planning, including various surveillance strategies, depending on the extent of disease and patient desire for treatment versus watchful waiting.
INTRODUCTION
Etiology
Cholesterol granuloma of the petrous apex is an acquired sterile inflammatory reaction to blood breakdown products resulting from cyclical bleeding and accumulation of cholesterol crystals into a pneumatized petrous apex. The bleeding may be from inflamed mucosa and/or leakage from the vascularized skull base marrow space (Figs. 11.9–11.11 and 113.1–113.4 and Chapter 11). This is now the most commonly diagnosed cystic expansile lesion of the petrous apex.
A mucocele occurs due to obstruction of an air cell tract leading to the petrous apex (Fig. 113.1). Continued secretions from the mucosa will lead to expansion of the petrous apex without bleeding. The obstruction may occur early in life since the slowly expansile, “cystic mass” appears to enlarge over a timetable measured in years (Figs. 113.5 and 113.6).
The main differential consideration is between these conditions and epidermoid cysts; the latter are discussed in detail in Chapter 8 (Figs. 8.7 and 113.7).
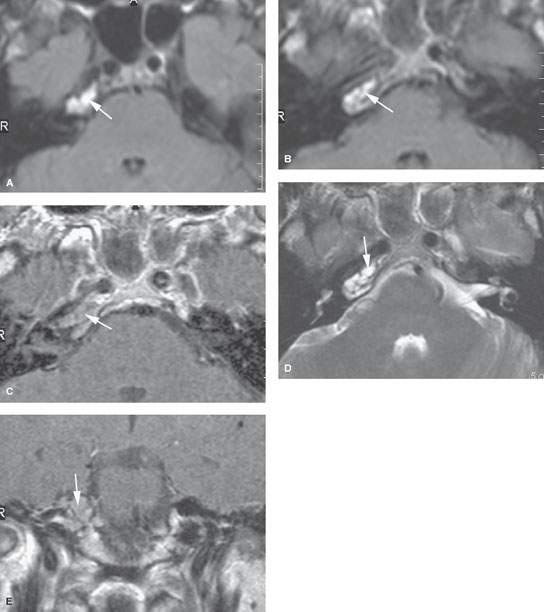
FIGURE 113.1. Magnetic resonance imaging (MRI) studies on a patient with an abnormal right petrous apex. A, B: The first MRI study on this patient done at another institution. In (A), the non–contrast-enhanced T1-weighted (T1W) image shows increased signal intensity at the right petrous apex (arrows). In (B), the contrast-enhanced T1W image shows the area to not change. No other images were available. From this study, it was uncertain about the nature of the petrous apex abnormality, which could have been anything from asymmetric aeration to a potentially progressive abnormality. C–E: Follow-up MRI study done at our institution. In (C), the contrast-enhanced T1W image shows the right petrous apex to be of generally increased signal intensity compared to the opposite side (arrow) and no definite abnormal dural enhancement. In (D), the air cells at the right petrous apex (arrow) clearly contain abnormal mucosa and/or fluid. The findings on the previous T1W images suggest that the fluid should be relatively mucoid or cholesterol laden. In (E), the coronal T1W image with contrast suggests a somewhat expansile appearance of the petrous apex confirmed by CT (not shown). (NOTE: Because of persistent right-sided headaches, the petrous apex was drained and the diagnosis of cholesterolosis was confirmed. It was difficult to be certain whether any of the increased signals on the contrast-enhanced T1W images was due to inflammatory enhancement.)
Prevalence and Epidemiology
Cholesterolosis and mucoceles are sporadic conditions with no known predisposing conditions except that the petrous apex must contain air cells and at some point there would need to have been an initial inciting insult. That initial event is typically not established by the patient history. Epidermoid cysts are developmental.
Clinical Presentation
Patients may present with otalgia and headaches leading to magnetic resonance imaging (MRI) or computed tomography (CT). The headache is typically retro-orbital or at the vertex. Occasionally, acute changes such as hemorrhage will produce a fifth or, more likely, sixth cranial nerve deficit (Fig. 11.11) in the absence of acute pyogenic infection. Secondary infection has not occurred in the experience of the authors. Also, hearing loss, vertigo, and tinnitus can occur. Petrous apex cholesterol granulomas, mucoceles, and epidermoid cysts may also be discovered on MRI studies of the brain done for possibly unrelated symptoms.
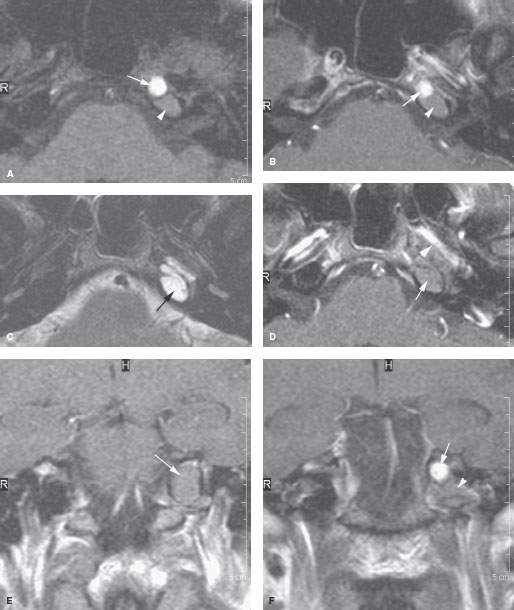
FIGURE 113.2. A patient with an abnormal left petrous apex as seen on magnetic resonance imaging. This is meant to demonstrate the range of abnormality that can be seen in cholesterolosis. A: Non–contrast-enhanced T1-weighted (T1W) fat-suppressed image showing a multiloculated process of brighter (arrow) and lesser (arrowhead) signal intensity. B: Contrast-enhanced T1W image showing no evidence of enhancement in either the brighter (arrow) or less bright component (arrowhead) or surrounding dura. C: T2-weighted image showing the entire abnormality to be of a relatively watery consistency, although the contents of the two different components likely are to be somewhat different in nature. D: A section somewhat lower showing no evidence of significant enhancement (arrow) and evidence of dehiscence of the carotid canal (arrowhead). E: Coronal section showing the overall cephalocaudal expansile nature of the mass (arrow). F: The coronal plane demonstrates the two components of brighter (arrow) and lesser (arrowhead) signal intensity components, although the less bright component is clearly different from cerebrospinal fluid. (NOTE: This was drained and confirmed as petrous apex cholesterolosis.)
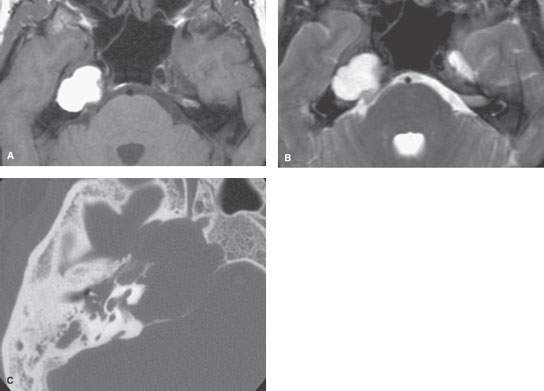
FIGURE 113.3. Abnormality of the petrous apex discovered on a magnetic resonance (MR) study done for a patient with headaches on the right side. A: Non–contrast-enhanced T1-weighted image showing an expansile mass of the petrous apex of increased signal intensity equivalent to that of fat or brighter. B: T2-weighted sequence demonstrating the relatively watery nature of the mass but showing no evidence of blood products or internal heterogeneity of the mass. C: Computed tomography study showing evidence of relatively low biologic activity with chronic remodeling of the bone of the petrous apex, including much demineralization of the carotid canal. (NOTE: Surgery revealed cholesterolosis. The opacification of the middle ear and mastoid visible on the MR study was due to the lesion occluding the bony eustachian tube.)
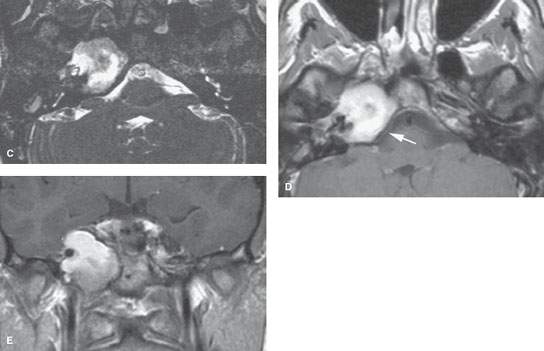
FIGURE 113.4. Magnetic resonance imaging study on a patient with surgically proven cholesterolosis. A: Non–contrast-enhanced T1-weighted (T1W) image showing the petrous apex mass to be of very bright signal intensity. B: T2-weighted image showing the lesion to be of mixed signal intensity with some particularly dark zones that could be due to hemosiderin deposition. C: A gradient echo acquisition from a CISS sequence emphasizes the heterogeneity within the area of abnormality, suggesting the presence of debris or possibly blood products. D: Contrast-enhanced T1W image showing no evidence of surrounding dural enhancement. E: Coronal T1W image with contrast shows that the more heterogeneous component was in the inferior part of the cholesterolosis, suggesting that there could be some collection or settling of the contents. (NOTE: This was drained, and cholesterolosis was confirmed with old blood products and cholesterol crystals identified.)
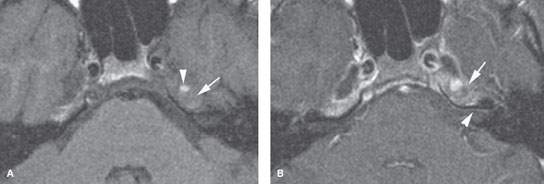
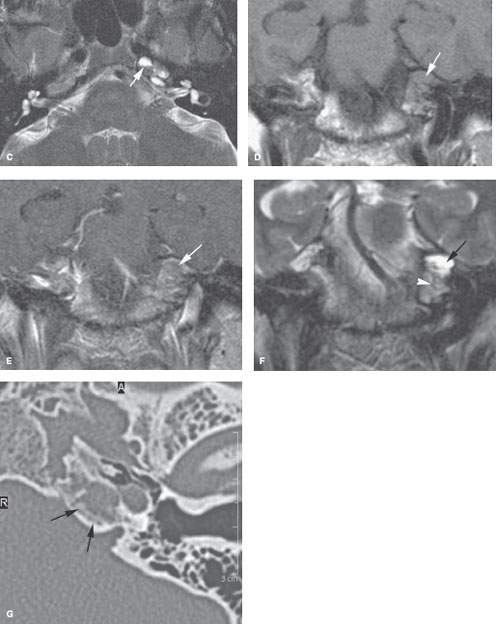
FIGURE 113.5. A patient with headaches and abnormal left petrous apex mass noted on magnetic resonance imaging. A: Non–contrast-enhanced T1-weighted (T1W) image showing the signal intensity of the petrous apex contents about isointense to brain (arrow) with a focal higher signal intensity component very similar to the situation illustrated in Figure 113.2. B: Contrast-enhanced T1W image showing definite evidence of enhancement of the process of the petrous apex and adjacent dural enhancement (arrow) even extending along the anterior wall of the internal auditory canal (arrowhead). C: T2-weighted (T2W) image showing a possible fluid–fluid level (arrow) and heterogeneity of contents of the petrous apex. D: Non–contrast-enhanced T1W image showing the overall cephalocaudal dimensions and signal intensity of the entire abnormality (arrow). E: Contrast-enhanced T1W image for comparison with (D) showing enhancement likely of the mucosa within the expanded petrous apex air cells (arrow). F: T2W coronal image showing a heterogeneity of the region, with the more superior aspect being of a more watery nature (arrow) compared to the more inferior component (arrowhead). G: Computed tomography image showing a possible chronic reactive bony change along the margin of the opacified petrous apex air cells rather than the relatively thin expansile appearance usually present in cholesterolosis. (NOTE: The lesion was drained, and chronically inflamed mucoid material was removed from the petrous apex. Final pathologic diagnosis was infected mucocele of the petrous apex without clear evidence of cholesterolosis.)
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Necrotizing (“Malignant”) Otitis Externa
Necrotizing (“Malignant”) Otitis Externa
 Cervicothoracic Junction: Brachial Plexus Trauma
Cervicothoracic Junction: Brachial Plexus Trauma
 Tumors of the Submandibular Gland and Space and Tumorlike Conditions
Tumors of the Submandibular Gland and Space and Tumorlike Conditions
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


