CHAPTER 8 Physics of Cardiac Computed Tomography
Computed tomography (CT) was first introduced in 1972 and has since become an indispensable tool for noninvasive diagnostic imaging. It is a robust and reproducible technique and its benefit for noninvasive cardiac imaging was soon envisioned and desired. Technical limitations prevented its applicability until the mid-1980s, but it was not until the introduction of multislice CT scanners with subsecond rotation times and higher volume coverage in the early 2000s1–3 that noninvasive cardiac CT imaging evolved into clinical routine.4–11 Among its various applications, coronary CT angiography (coronary CTA) has emerged as a valuable tool for imaging the coronary arteries, for which it has been shown to quantify coronary artery stenosis with high accuracy and especially to have a high negative predictive value for coronary artery disease (CAD). Imaging the heart and coronary anatomy poses high demands on spatial and temporal resolution. The small coronary arteries, with diameters typically of 2 to 4 mm, require optimal image quality and maximum resolution for reliable visualization and analysis. Because of their location close to the heart muscle and consequent strong movement during the cardiac cycle, their imaging requires almost freezing the heart to avoid motion artifacts. Finally, the scan time for covering the complete heart volume should be within the time of a single breath-hold to avoid breathing artifacts and limit radiation exposure and amount of contrast administered.
First introduced in 2004,12 64-slice CT systems helped establish CT imaging of the heart in clinical routine and were until recently considered state of the art. This section will therefore focus on 64-slice CT because it is still the widest available technology. The most recent developments, such as dual-source CT with high-pitch scanning and volume acquisition CT scanners, are expected to improve cardiac imaging further. These will be discussed at the end of this chapter.
CARDIAC IMAGING REQUIREMENTS
Two goals can generally be defined for cardiac imaging. First, the imaging modality should allow virtual “freezing” of the motion of the heart to avoid motion artifacts. The time interval of the cardiac cycle contributing to an image should be short enough to allow the depiction of at least slow motion heart phases without motion artifacts. Second, the imaging technique should allow the selection of defined heart phases of the cardiac cycle. Because motion intensity varies over the heart cycle, with the slowest motion (usually) present in the diastolic phase, imaging is typically performed during this phase of the cardiac cycle to minimize image blurring caused by motion. A temporal resolution of 250 ms is generally considered sufficient for motion-free imaging for slow to moderate heart rates of up to 65 beats/min, because the length of the diastolic phase shortens with increasing heart rate.13 However, if imaging is desired for phases other than diastole (e.g., for functional information), more stringent requirements are necessary. Posing very rigorous demands on image quality, such as motion-free imaging in all heart phases, would require a temporal resolution shorter than 50 ms.
IMAGE RECONSTRUCTION TECHNIQUES FOR OPTIMIZED TEMPORAL RESOLUTION
The optimal temporal resolution is achieved with algorithms that use the minimum amount of required data for image reconstruction.2,3,14 Generally, CT image reconstruction requires at least a parallel projection data angle range of 180 degrees. As a consequence, the temporal resolution will be on the order of trot/2, where trot is the time required for a full rotation of the scanner. However, the temporal resolution varies with the position in the scan field of view, which is determined by the temporal interval covered by the data contributing to the reconstruction to a particular image point. In a centered region of the scan field of view, the temporal resolution equals half the rotation time. In clinical practice, the heart should be sufficiently centered during data acquisition to maintain stable temporal resolution of half the rotation time. Half-scan reconstruction techniques preserve the spatial resolution compared with standard reconstructions, but because of less data contributing to an image, the noise is usually increased by a factor of  . Special considerations apply to today’s third-generation modern CT scanners, in which data acquisition is performed in fan beam geometry. Data is acquired over a range of 180 degrees plus fan angle and is then transformed to parallel beam geometry using so-called “rebinning techniques.” The previously described half-scan reconstruction algorithm is then applied to achieve the best temporal resolution.
. Special considerations apply to today’s third-generation modern CT scanners, in which data acquisition is performed in fan beam geometry. Data is acquired over a range of 180 degrees plus fan angle and is then transformed to parallel beam geometry using so-called “rebinning techniques.” The previously described half-scan reconstruction algorithm is then applied to achieve the best temporal resolution.
With the introduction of multislice helical CT, almost isotropic three-dimensional resolution became feasible. Dedicated reconstruction algorithms are necessary to optimize temporal resolution, helical artifact reduction, and volume coverage. The basic concepts for phase-correlated imaging for multislice CT have been introduced with four-slice systems1,15 and are used in slightly different forms in today’s scanners.
Modern 64-slice CT scanners all offer rotation times of less than 0.5 second and down to 0.3 second. Thus, it is possible to achieve a temporal resolution of 150 ms, which allows for motion-free imaging in the diastolic phase for moderate to high heart rates. As a consequence, the usage of β blockers, intravenous or oral, to slow down the heart rate is common practice.8 Nevertheless, motion artifacts remain the most important challenge for coronary CTA, even with 64-slice CT systems.
ECG Synchronization
Traditionally, the patient’s electrocardiogram (ECG) has been used to correlate acquisition and reconstruction of CT data with heart motion. Data can be acquired in phases with slow motion to minimize motion artifacts; alternatively, the acquisition and reconstruction of different heart phases are possible for functional studies. Usually, the R wave of the ECG is used as a reference point, with the R wave being the most pronounced peak in the ECG. Alternative approaches to derive the motion signal retrospectively have been proposed, using information from CT raw data directly or from the generated images.16 However, for phase-correlated data acquisition, the ECG signal is used.
The start point of data acquisition or, respectively, data selection for image reconstruction is usually determined relative to the R waves of the ECG signal by a phase parameter. Three phase selection strategies are commonly used (Fig. 8-1)—relative delay (e.g., at 65% of the R-R interval), absolute delay, and absolute reverse (e.g., 400 ms after and before the R wave, respectively). For the relative delay, a temporal delay relative to the start point of the previous R wave is used to determine the start point of the ECG-triggered acquisition or the data reconstruction interval. This delay is determined individually for each heart cycle. For prospective data acquisition, the R-R interval times have to be prospectively estimated based on prior R-R intervals. The absolute delay uses a fixed delay time after onset of the R wave to trigger the data acquisition or start point of the reconstruction. Absolute reverse describes a fixed time prior to the onset of the next R wave for starting data acquisition or the start point of the reconstruction interval. For ECG-triggered data acquisition, the position of the next R wave again has to be estimated from previous R-R interval times.
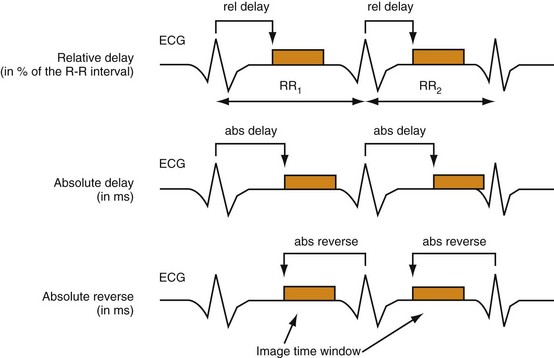
 FIGURE 8-1
FIGURE 8-1TECHNICAL PRINCIPLES OF CARDIAC IMAGE ACQUISITION
Prospective Triggering
Prospective triggering uses the ECG signal to start the scan (data acquisition and x-ray on time). This technique is typically used with axial scans, meaning that the patient table is at rest during data acquisition. For imaging, the user specifies the delay time after the R wave; usually, the scan delay time is selected so that the data are acquired during the diastole of the heart. For each position, the scanner is continuously rotating until the ECG trigger signal indicates the desired heart phase, when the x-ray is switched on and data are acquired for 180 degrees plus the fan angle. The number of reconstructed images corresponds to the number of detector rows used. With the x-ray then switched off, the table advances to the next position, which typically corresponds to the total detector collimation (slight overlaps are necessary for contiguous volume coverage). This is repeated until the heart range is covered; thus, the technique is commonly referred to as a “step-and-shoot mode” (Fig. 8-2). Image reconstruction is performed with previously described half-scan algorithms, and so the temporal resolution corresponds to half the rotation time.
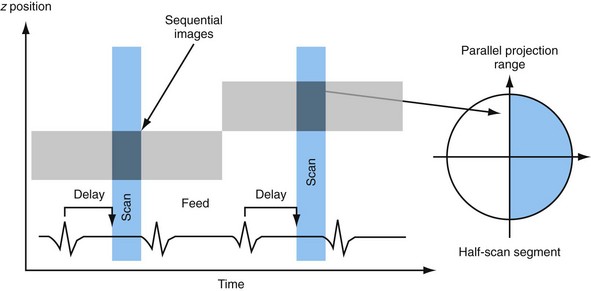
 FIGURE 8-2
FIGURE 8-2However, cardiac CT examinations have recently been subjected to increased scrutiny because of their relatively high radiation dose.17,18 Prospective triggered data acquisition offers the highest dose savings and hence has experienced renewed interest.19–21 In addition, improvements in ECG synchronization, such as so-called adaptive triggering or padding techniques, allow the system to react to ectopic beats and allow image reconstruction in a narrow phase range beyond the specified acquisition phase.
Retrospective Gating
With submillimeter slice thickness, 64-slice CT offers considerable advantages over earlier technology in terms of spatial resolution and volume coverage. Two different scanner concepts were introduced. The volume concept provides a further increase in volume coverage by increasing the number of detector rows to 64. The resolution concept uses 32 physical detector rows in combination with double sampling in the longitudinal z direction. Thus, 64 overlapping slices are simultaneously acquired to increase longitudinal resolution independently of the pitch and reduce helical artifacts.12
With the advent of multislice helical CT scanning, various image reconstruction concepts have been introduced to take full advantage of volumetric ECG-gated data acquisition.1,14 The reconstruction process typically comprises two steps. The first step generally involves multislice helical interpolation algorithms to compensate for the continuous table movement during data acquisition. The second step uses half-scan reconstruction techniques for the generated transverse data segments to optimize temporal resolution.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


