Fig. 27.1
Abdominal ultrasound in a 34-year-old male with history of Crohn’s disease and enterocutaneous fistula in the mid-abdomen. This patient presented with new drainage of pus from a new skin site, with ultrasound demonstrating two fistulous tracts to the skin surface with pus drainage, compatible with enterocutaneous fistulas
Fistulogram
Traditionally, fistulography has been the most rapid and widely used technique in the evaluation of communication between the skin opening and bowel or abdominal cavity (Fig. 27.2). During fistulography, the external skin opening is cannulated, followed by injection of a water-soluble contrast agent under fluoroscopic guidance to delineate the fistulous tract. Multiple fluoroscopic images are usually obtained in various obliquities by moving the patient in different positions to allow for dependent drainage and improved visualization. Using this thorough technique the location of the fistula, length of the tract and extent of the bowel wall disruption can be adequately evaluated. Water-soluble agents such as Gastrografin have the advantage of rapid absorption within the peritoneal cavity while causing minimal inflammation. However, Gastrografin usually provides less mucosal detail compared to barium. Therefore, a water-soluble iodinated contrast agent is often injected initially, followed by barium if no extravasation is seen and additional detail is required. While a cost-effective and efficient diagnostic test, a fistulogram may still fail to provide detailed information regarding contained abscess collections, exact location of the fistula in the GI tract, or additional bowel pathology proximal or distal to the fistula. Fistulography is also contraindicated in patients with sepsis, as the technique may result in bacteremia. If the result of fistulogram is inconclusive, additional imaging studies such as a small bowel follow-through, CT, or MRI can be performed.
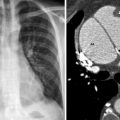
Fig. 27.2




Plain film image of a fistulogram in a 23-year-old male with history of gunshot wound to the abdomen and ileostomy depicting an enterocutaneous fistula communicating with the jejunum and antegrade flow of the contrast towards the ileostomy site. The contrast opacification pattern suggests the fistula arising from the mid jejunal loops, proximal to the ileostomy. Of note, the image also shows the patients hand; he was asked to hold the catheter firmly during injection of the contrast
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
