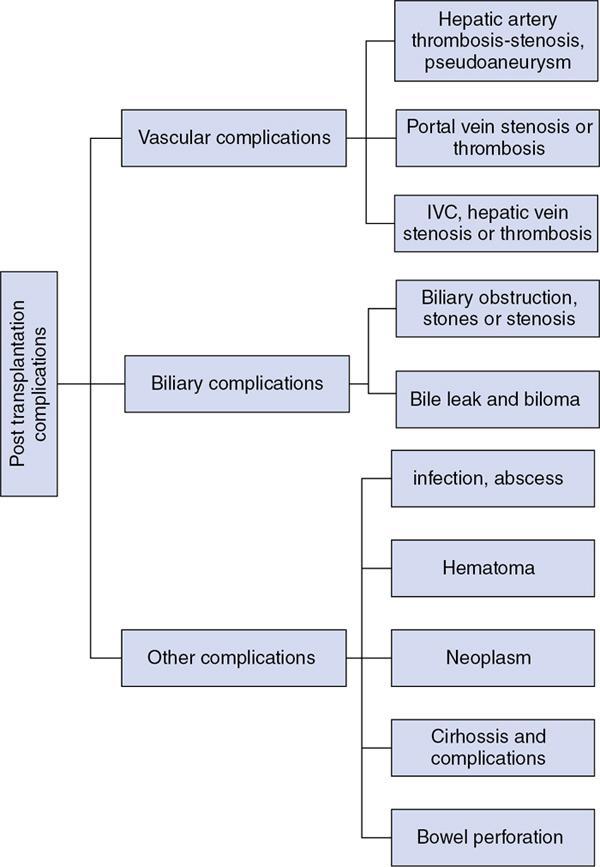
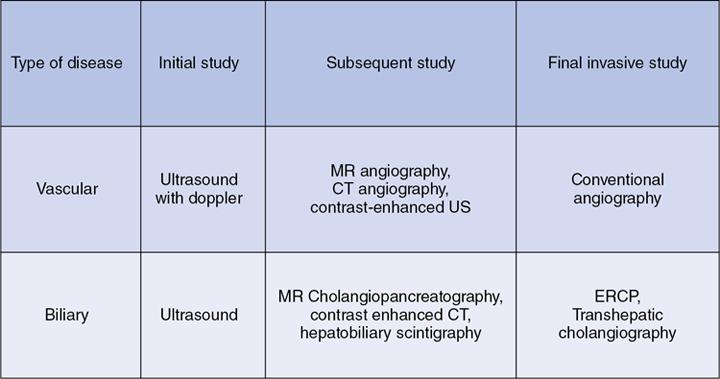
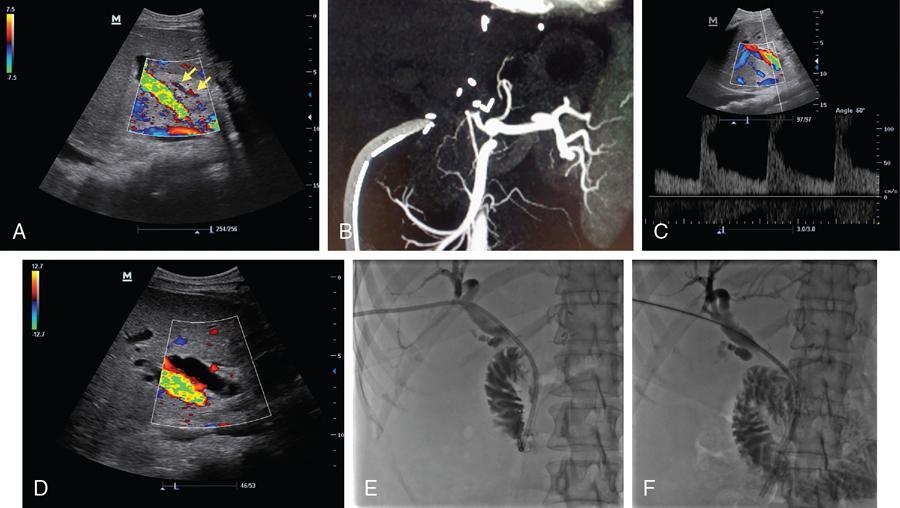
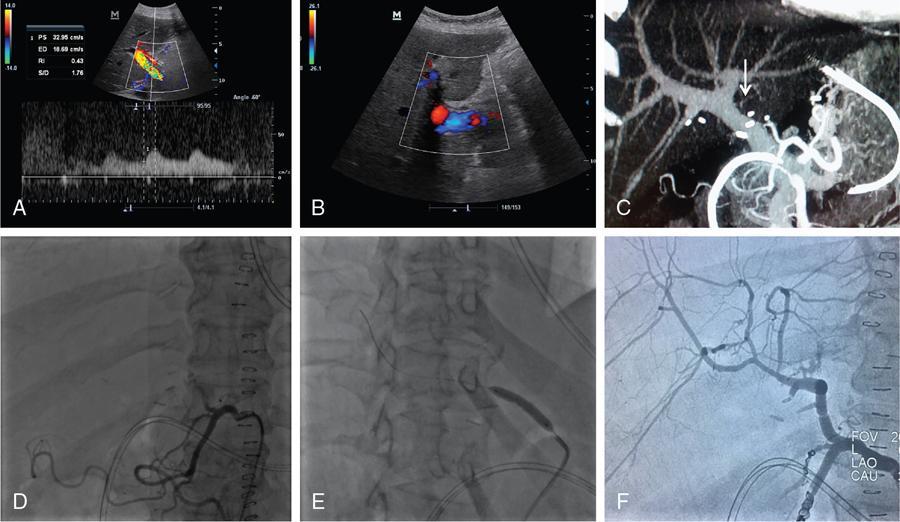
M.C. Uthappa, Soumil Singhal Liver transplantation is performed in patients with end-stage liver disease or patients with acute liver failure. The world’s first liver transplantation was performed by Dr. Thomas Starzl in 1963. Thousands of transplant surgeries are being performed in India every year. Each transplant reflects an outstanding benevolence of the donor and the family. However, India still ranks quite low in the organ donation program, because of which several patients are waiting on the transplant list eagerly. Transplantation surgery is a multidisciplinary approach involving surgeons, physicians, anaesthetists and nursing teams who work through the complexity to achieve a good result in every patient. The evolution in the operational technique and intensive care units have helped reduce both morbidity and mortality rates, resulting in improved survival outcomes. Orthotopic transplantation is the commonly performed technique that is performed on the adult and paediatric populations worldwide. Despite advancements in transplantation surgery, complications are inevitable in some clinical scenarios. Both diagnostic and intervention radiology plays a vital role in different phases of the procedure. Interventional Radiology is a subspecialty of radiology that offers treatment options with minimal invasion. This chapter covers the role of interventional radiology in various clinical scenarios presented in patients undergoing liver transplant surgery. A successful liver transplant normally involves three major vascular reconstructions including the hepatic artery, inferior vena cava, and portal vein. The portal vein and hepatic artery are commonly reconstructed using an end-to-end anastomosis. Inferior vena cava is commonly reconstructed using a piggyback technique (end to side anastomosis). These vascular anastomoses are associated with higher morbidity and mortality risks. Patients usually present with these complications within three months of surgery. Posttransplantation complications have always been a matter of concern to the transplant surgeon. It can involve the arterial/venous structures, the biliary system, or even the liver parenchyma itself. Recipients are closely followed up using noninvasive techniques to rule out any complications. Fig. 9.29.1 briefly categorizes the various complications associated with the surgery (Fig. 9.29.2). Serious complications can end up leading to retransplantation. Interventional radiology has played a vital role in the multidisciplinary transplant team. They have been an essential component in a good transplant program worldwide. The continued advancement in technology and the gamut of technical skills have allowed in managing many complications without the need for surgery. These include (a) hepatic artery thrombosis (HAT), (b) hepatic artery stenosis (HAS), and (c) hepatic artery pseudoaneurysm. HAT is one of the most common vascular complications which is seen in up to 12% of cases. It can present as early as on the 2nd postoperative day following transplantation and is a cause of early postoperative graft failure or mortality. As the hepatic artery provides essential blood supply to the biliary ducts, thrombosis leads to biliary ischemia, bile leak, sepsis, hepatic necrosis, and graft failure. Clinically patient presents with complaints of pain, fatigue, fever, leukocytosis and raised liver function parameters. Postoperative Doppler ultrasound plays a vital role due to high sensitivity and specificity for the detection of HAT. However, it can cause false positive and false negative diagnoses. False-negative is seen in patients with subacute or late HAT presenting with collaterals and false-positive in cases with low cardiac output, parenchymal oedema or vasospasm of the vessel. Doppler shows a loss of arterial signal which is a highly sensitive feature. A raised resistive index is also seen proximal to a thrombosis. A CT or MR angiography is performed to confirm the diagnosis which has high sensitivity and specificity. Contrast-enhanced ultrasound can also be performed to detect an absence of flow. The various treatment options available for the patients include retransplantation, surgical revascularization and endovascular revascularization. Surgical revascularization is found to be effective in early HAT, however, in case of extensive thrombosis endovascular approach is helpful. Endovascular revascularization is performed in HAT presenting in the late 1st week to 3rd week. The various endovascular treatment options include catheter-directed thrombolysis, transluminal angioplasty, and stent placement. Hidalgo et al. in 1989, first demonstrated the use of catheter-directed thrombolysis in HAT. Thrombolysis is performed by an initial bolus of urokinase followed by a continuous infusion. A single bolus sometimes does not completely clear the thrombus load requiring a prolonged infusion (Figs. 9.29.3 and 9.29.4). Haemorrhage is the most common complication for which close monitoring of the abdominal drains, coagulation parameters, and haemoglobin is warranted in this setting. Thrombolysis may unmask the underlying cause which may require angioplasty or stenting. Catheter-directed thrombolysis is a salvage procedure which needs further research to ascertain long term outcomes. Splenic artery steal syndrome: Another clinical situation known as Splenic artery steal syndrome can deviate blood from the graft leading to hepatic artery thrombosis. A better understanding of this condition has associated this condition to portal vein hyperperfusion (PVHP) in patients with uncompensated severe portal hypertension. The hepatic artery buffer response reduces the hepatic artery flow in these patients leading to thrombus formation. Suspicion of PVHP is raised when there is high intraoperative portal vein flow (>2 cc/g/minute), improvement of intraoperative hepatic artery flow on portal vein occlusion, and failure in the normalization of the hepatic artery RI with deranged liver parameters. Conventional hepatic artery angiogram shows complete hepatic artery occlusion. This can be corrected by proximal splenic artery embolization. Embolization of the splenic artery reduces the portal pressure allowing a reduction in hepatic artery RI and reestablishing a forward flow. Materials required before the procedure: It is the second most common complication seen in about 2%–11% of transplant patients. It is an early complication and has a median time of about 100 days. The most common site of stenosis is at the anastomotic site. Doppler ultrasound shows an increased peak systolic velocity (>200 cm/second) at the site of the stenosis. Distally arteries show a tardus-parvus waveform with a low Resistive Index (<0.5) and long systolic acceleration time (>0.08 seconds). Gradual decrease in RI on successive scan is an indicator of thrombosis. CT angiographic allows reliable identification of HAS as a focal narrowing as a confirmatory form of imaging or as a problem-solving tool. MR angiography is limited by relatively high false-positive rates. HAS may be treated with surgical intervention or percutaneous angioplasty and/or stenting. Studies have shown both angioplasty (Fig. 9.29.4) and stenting to have comparable high technical success rates with low complication rates. Complications related to the procedure include dissection, arterial rupture, HAT, and restenosis. These patients need to be on continued clinical and imaging follow up for patency assessment. Materials required before the procedure:
9.29: Postliver transplant complications and interventions
Introduction
Posttransplant complications
Vascular complications
Hepatic artery complications
Hepatic artery thrombosis
Hepatic artery stenosis
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Postliver transplant complications and interventions






