PRESEPTAL COMPARTMENT: ACUTE AND CHRONIC INFECTIONS AND NONINFECTIOUS INFLAMMATORY CONDITIONS
KEY POINTS
- Imaging is not required in the vast majority of patients with acute and chronic infections and noninfectious inflammatory conditions of the preseptal compartment.
- Imaging can be used to identify possible sources of infection and complicating factors that will alter medical decision making in selected cases.
- Imaging can help exclude dangerous confounding factors such as a mass leading to secondary inflammatory changes.
Any orbital mass or disease process may be approached by first establishing whether it is preseptal (Chapters 70 and 71) or postseptal (Chapters 57–60, 62, and 64). Preseptal problems most commonly arise from the skin, eyelids, lacrimal gland (Chapter 65), and nasolacrimal drainage apparatus (Chapters 68 and 69), all of which are components of the preseptal space. The vast majority of these problems do not come to imaging. This chapter considers preseptal inflammatory processes, which arise from sources other than the lacrimal gland and nasolacrimal drainage system, and those arising in this location that might spread across the orbital compartments and related spaces.
Noninfectious inflammatory diseases may be local or related to systemic disease. Practically, the preseptal space is only secondarily involved in diseases such as sarcoidosis and Wegener granulomatosis and autoimmune disease that arises at other sites. Infections, like noninfectious inflammatory conditions, may be local or related to systemic disease. The vast majority of these conditions arise in the skin and eyelid, with few due to secondary spread from conditions of the sinonasal region (Chapters 84–86), lacrimal gland (Chapter 65), and lacrimal drainage system (Chapter 68).
ANATOMIC AND DEVELOPMENTAL CONSIDERATIONS
Applied Anatomy
The relevant anatomy of the preseptal soft tissues, orbital septum, lacrimal gland, and nasolacrimal drainage system is discussed in detail in Chapter 44.
IMAGING APPROACH
Techniques and Relevant Aspects
The preseptal soft tissues are studied with computed tomography (CT) and magnetic resonance (MR) techniques described in detail in Chapters 44 and 45. Specific CT protocols by indications are detailed in Appendix A. Specific MR protocols by indications are outlined in Appendix B. Almost all studies to investigate potential preseptal inflammatory pathology are done with contrast.
Pros and Cons
Disease of the preseptal soft tissues is studied primarily with CT, with magnetic resonance imaging (MRI) held in reserve for highly selected cases.
CT typically is used to identify bone changes and exclude abscess or a deeper underlying source of the inflammation.
Dacryocystography and dacryoscintigraphy are used in conjunction with diseases that arise in the lacrimal drainage system (Chapter 68).
Ultrasound is of no real clinical decision-making benefit.
SPECIFIC DISEASE/CONDITION
Noninfectious Inflammatory Disease
Etiology
Noninfectious inflammatory diseases may be local or related to systemic disease. The preseptal soft tissues may be secondarily involved with granulomatoses and histiocytoses that infiltrate those tissues from other preseptal sources such as the lacrimal gland and drainage system, postseptal orbit, and sinonasal tract that appear identical to lymphoma.1 These diseases are discussed in general in chapters on sarcoidosis (Chapter 18), Wegener granulomatosis (Chapter 17), and Langerhans histiocytosis (Chapter 19). Pseudotumor and primary acquired nasolacrimal duct obstruction may also secondarily involve the entire or portions of the preseptal space (Chapters 18, 57, and 68).
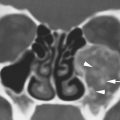
Preseptal inflammation may also be due to insect bites and toxic exposures. As well, it may be due to relative nonspecific conditions such as angioneurotic edema and more rare conditions such as Kimura disease2 (Fig. 70.1).
Clinical Presentation
These processes appear as soft tissue swelling. Localization more medially suggests a sinonasal or nasolacrimal system origin, and a superior lateral localization suggests a lacrimal gland origin.
Pathophysiology and Patterns of Disease
These conditions produce inflammation and various degrees of swelling spreading in the preseptal soft tissues. The pathophysiology of these inflammatory is discussed in Chapter 13.

FIGURE 70.1. A patient presenting with preseptal soft tissue swelling of unknown cause. This computed tomography study shows extensive preseptal soft tissue swelling (arrows) limited by the attachment of the orbital septum (arrowhead). Biopsy finally showed Kimura disease.
Manifestations and Findings
Computed Tomography and Magnetic Resonance Imaging
CT and MRI may show discreet but more usually generalized soft tissue swelling and the relationship of the pathology to the orbital septum (Figs. 44.17 and 70.1). It may show bony erosion along the attachments of the septum to the lacrimal and other bones. Bone changes at the points of attachment of the orbital septum may not be apparent on MRI since this is essentially cortical bone being demineralized. The CT and MRI findings in inflammatory disease are discussed in general in Chapters 13 and 16 and with regard to sarcoidosis (Chapter 18), Wegener granulomatosis (Chapter 17), and Langerhans histiocytosis (Chapter 19) in chapters as noted. Those specifically arising in the nasolacrimal system (Chapter 68), lacrimal gland (Chapter 65), and sinonasal region (Chapters 84–86) are discussed in chapters as noted.
Nuclear Medicine
Dacryoscintigraphy may be used to noninvasively determine if the lacrimal drainage system is blocked as a primary source or secondary effect of the pathology. Obstruction may be generally characterized by such study as proximal to the lacrimal sac, at the sac–duct junction, or a distal duct obstruction (Chapter 68).
Differential Diagnosis
From Clinical Data
Distention of the lacrimal sac together with tearing and pain and inflammation in the medial canthal area strongly suggest a nasolacrimal drainage system origin. Signs and symptoms of sinonasal disease suggest that origin. Localization to the upper outer orbital quadrant suggests a lacrimal gland or possible frontal bone or sinus origin. Otherwise, the process likely arises from the skin.
From Supportive Diagnostic Techniques
Diagnostic imaging with CT or MRI is pivotal for confirmation of whether the process is likely a primary inflammatory one and limited to the preseptal soft tissues. Imaging is instrumental in excluding a postseptal, sinonasal, and/or lacrimal system origin or extension of the pathology.
Biopsy is used very selectively if a tumor is strongly suspected (Fig. 70.1).
Medical Decision Making and Treatment Options
Medical
If noninfectious inflammatory disease is identified, steroid or immunosuppressive therapy may also be instituted.
Surgical
If causative pathology in the sinuses or lacrimal drainage system is identified, surgery may include tissue sampling and relief of obstruction.
DISEASE ACUITY AND REPORTING RESPONSIBILITY
These are typically routine studies that may be reported routinely.
The report should clearly identify whether this is a disease confined to the preseptal soft tissues or one that has a postseptal component. It should also identify possible sinonasal, lacrimal drainage system or lacrimal gland origin and exclude a contributing mass with as high a degree of confidence as possible. It should also comment on the presence or absence of factors that might contribute to identify the etiology such as orbital, ocular, or intracranial findings suggestive of systemic disease such as Wegener granulomatosis, Langerhans cell histiocytosis, or sarcoidosis.
Related posts:
 Fibrous Dysplasia and other Fibro-osseous Lesions of the Craniofacial Skeleton
Fibrous Dysplasia and other Fibro-osseous Lesions of the Craniofacial Skeleton
 Intraconal Orbit: Tumors
Intraconal Orbit: Tumors
 Hypopharynx: Developmental Abnormalities
Hypopharynx: Developmental Abnormalities
 Tumors of the Submandibular Gland and Space and Tumorlike Conditions
Tumors of the Submandibular Gland and Space and Tumorlike Conditions
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


