| Skull Base Region | Left sella turcica and left cavernous sinus |
| Histopathology | N/A |
| Prior Surgical Resection | Yes |
| Pertinent Laboratory Findings | Prolactin: 200 ng/mL |
Case description
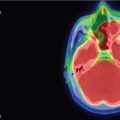
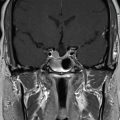
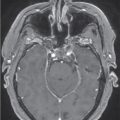
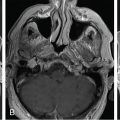
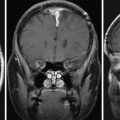
A 35-year-old female with a 3-month history of amenorrhea was found to have prolactin levels elevated to 200 ng/mL. Imaging revealed a left-sided pituitary microadenoma ( Figure 3.15.1 ). She was started on cabergoline 0.25 mg twice a week, and her prolactin subsequently dropped to 140 ng/mL. Her cabergoline regimen was increased to three times weekly, but this dose did not result in normal prolactin levels. Imaging obtained a year later showed interval growth of the tumor along the left side of the sella turcica, contiguous with the wall of the left cavernous sinus. She was diagnosed with a medically resistant prolactinoma and was referred for surgical excision via a sublabial microscopic transsphenoidal approach. The sellar portion of the tumor was fully excised, although the lateral aspect was found to have likely dural invasion, and residual tumor was left within the left cavernous sinus ( Figure 3.15.2 ). Postoperatively, her prolactin levels dropped to 70.5 ng/mL but were still elevated, so she was referred for stereotactic radiosurgery (SRS) ( Figure 3.15.3 ).
| Radiosurgery Machine | Gamma knife |
| Radiosurgery Dose (Gy) | 25, at 50% isodose line |
| Number of Fractions | 1 |



| Critical Structure | Dose Tolerance |
|---|---|
| Optic nerve/chiasm |
|
| Brainstem |
|
| Cranial nerves in cavernous sinus |
|
| Cavernous carotid artery |
|
| Normal pituitary gland and pituitary stalk | Recommend to limit radiation exposure to the identifiable gland to <11.0 Gy and to avoid whole-sella SRS whenever possible |
Related posts:
 Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
 Null cell – delayed postoperative radiosurgery for growing perioptic residual
Null cell – delayed postoperative radiosurgery for growing perioptic residual
 Chordoma – immediate postoperative/post-proton therapy radiosurgery for residual disease
Chordoma – immediate postoperative/post-proton therapy radiosurgery for residual disease
 Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
 Capillary hemangioma – postoperative radiosurgery for residual tumor
Capillary hemangioma – postoperative radiosurgery for residual tumor
 Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


