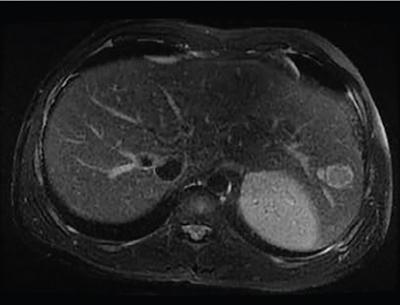
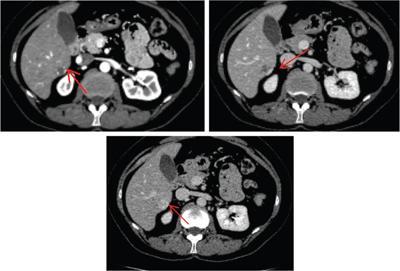
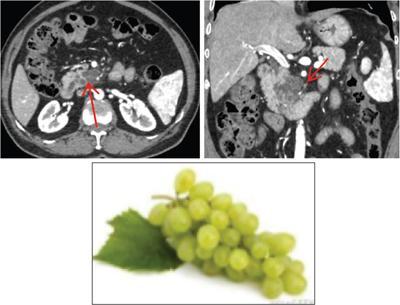
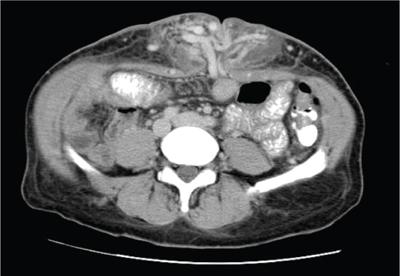
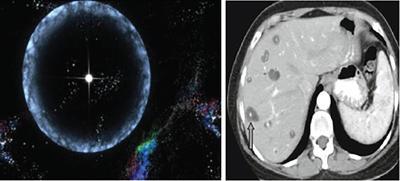
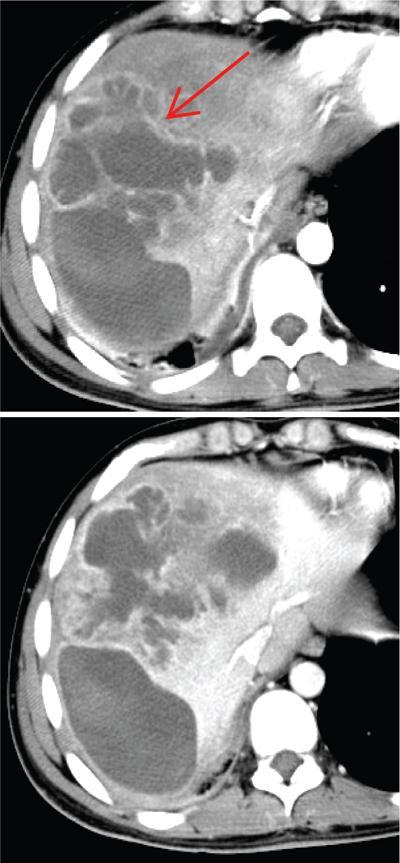
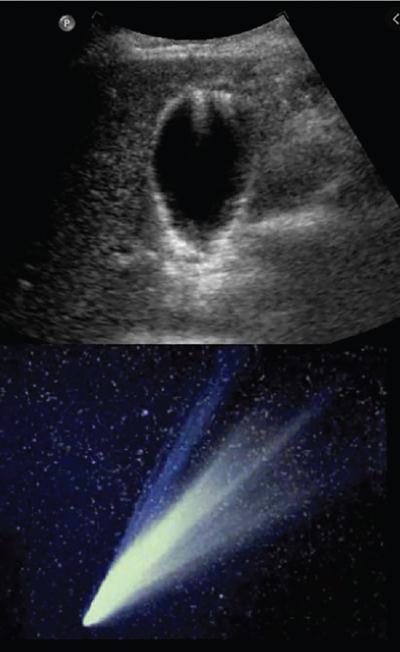
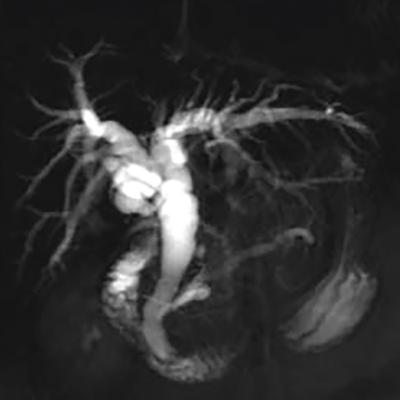
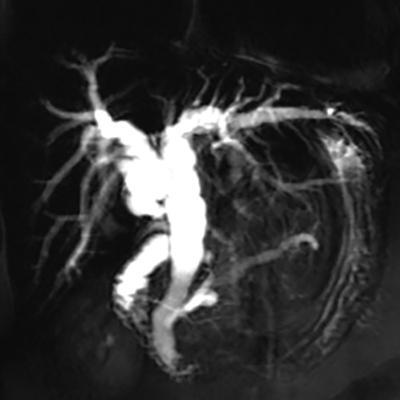
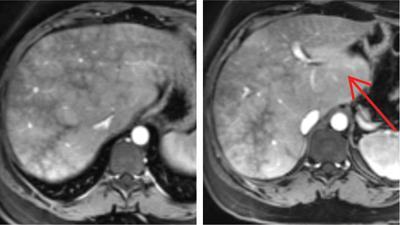
Shrinivas B. Desai, Ritu K. Kashikar, Shreya Shukla Radiological signs are classical and distinctive abnormalities characteristic of a disease. These can be seen on any imaging modality. Resemblance to commonly seen objects and patterns form the basis of radiological signs. The aim is to help the reader associate, understand and memorize these pathologies with the aid of signs. Various signs pertinent to hepatobiliary system are described in the chapter. Described on MRI when liver lesion shows a peripheral rim of high T2 signal intensity with the centre of the lesion appearing isointense to the background of noncirrhotic liver on T2WI mimicking an atoll. It is considered a characteristic sign of an inflammatory hepatic adenoma (image) but is only seen in about one-third of cases Extrinsic smooth impression over medial aspect of duodenum along its posteroinferior aspect, seen in pancreatic head pathologies like carcinoma. This sign is seen in pancreatic adenocarcinoma Presence of a persistently hyperattenuating dot within a lesion on arterial and portal venous CT. This corresponds with peripheral nodular enhancement seen on dynamic MR. Presence of bright dot suggests that the lesion is a hemangioma and helps in ruling out metastasis Ultrasound appearance of multiple cystic spaces or lesions that has been used to describe the appearance of an intraductal papillary mucinous neoplasm of the pancreas. Seen on contrast CT in portal hypertension. The appearance is based on resemblance to Medusa from Greek mythology. Dilated engorged paraumbilical veins radiating across umbilicus to join systemic veins is seen. This sign is seen in Caroli’s disease on contrast CT. Enhancing dots within dilated intrahepatic bile ducts represent portal radicles. Caroli’s disease Irregularly dilated pancreatic duct with multiple strictures and intervening dilatation with associated dilated side ductules resemble multiple lakes supplied by a single territory. Best seen in MRCP images. Chronic pancreatitis It is a finding on MRI and CT and is best seen on MRI T2-weighted and postcontrast T1-weighted sequences. Small necrotic/purulent areas in the pyogenic abscess ‘cluster’ together and then coalesce into a larger necrotic/purulent areas, eventually becoming a larger septated abscess cavity. At the periphery of these clusters: Associated with pyogenic hepatic abscesses and can help differentiate pyogenic abscesses from other types of liver lesions Abrupt termination of gas within the proximal colon at the level of radiological splenic flexure. The inflammatory exudates in pancreatitis extend to the phrenicocolic ligament giving rise to this sign Seen on grey scale ultrasound as a reverberation artifact when small calcific or highly reflective objects are imaged. The colour comet-tail artifact is an ultrasonographic sign seen in a number of situations when colour Doppler scanning is performed. This sign occurs in cases of traumatic right-sided diaphragmatic rupture with resultant partial herniation of liver through the defect. Separation of the herniated liver from its intra-abdominal component is via a small constriction at the level of diaphragm resembling a cottage loaf. Cottage loaf is a particular shape of bread in which larger and smaller roughly spherical balls are squashed together. Traumatic right-sided diaphragmatic rupture with resultant partial herniation of liver Bile eccentrically outlines luminal stone, creating a low attenuation crescent. Best seen on MRCP images. Choledocholithiasis Dilatation of both pancreatic duct and CBD is referred to as the double duct sign. Positive double duct sign suggests the diagnosis of carcinoma of the head of the pancreas and ampullary tumours and is hence considered ominous. Occasionally the sign may be seen in impacted gallstone in the distal duct. This feature is seen in patients with liver abscess on contrast-enhanced CT. A double, inner hyperattenuating and outer hypoattenuating rim is seen surrounding the hypodense abscess. The inner hyperattenuating rim corresponds to the enhancing abscess membrane, while the outer rim corresponds to the edema of the surrounding liver which appears hypodense and may show delayed enhancement. Liver abscess A positive duct penetrating sign is when a mass is penetrated by an unobstructed pancreatic duct; this makes focal pancreatitis the most likely cause rather than pancreatic carcinoma. This sign is best appreciated on MRCP (or ERCP). A radiographic sign that can be useful in differentiating between focal pancreatitis (inflammatory pancreatic mass) from pancreatic carcinoma. The duct-penetrating sign on MRCP is more helpful in differentiating between these two entities than a delayed enhancement pattern on CT or MRI It occurs when there is both limy bile and a gallstone in the common bile duct. The linear vertical radiopaque bile forms the line of the exclamation mark (i.e. !), whilst a more distal calculus forms the ‘dot’ at the end of the exclamation mark. Pathognomonic imaging sign of the rare diagnosis of limy bile on plain abdominal radiography Nonenhancing ruptured lesion with peripheral rim enhancement showing discontinuity from the rest of the liver and protruding from the liver surface is called the enucleation sign. Ruptured HCC Enlargement of the pericholecystic space. One of the signs of liver cirrhosis Can be seen on technetium 99m sulphur colloid scans of the liver and spleen, as well as CT studies. It occurs as a focal area of increased radiopharmaceutical uptake in the medial segment of the left hepatic lobe (segment IV) occurring as a result of SVC obstruction and portosystemic venous shunting between the superior vena cava and the left portal vein via the internal thoracic and paraumbilical veins. The equivalent of this sign may also be seen on contrast-enhanced CT scans as a hypervascular region. Budd–Chiari syndrome causes the hot spot sign in the caudate lobe
9.5: Radiological signs – hepatobiliary system
Name of the Sign
Description/Reason for the Appearance
Image With or Without Illustration
Causes and Significance
1) Atoll sign

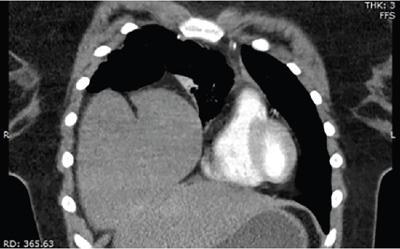
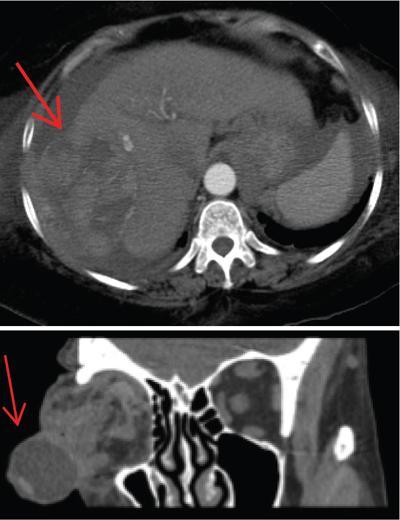
2) Antral pad sign
3) Bright dot sign
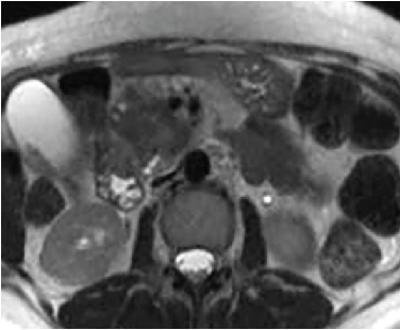
4) Bunch of grapes sign
5) Caput medusae sign

6) Central dot sign
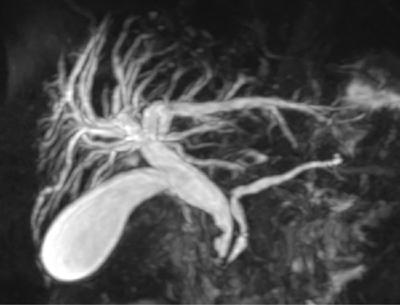
7) Chain of lakes

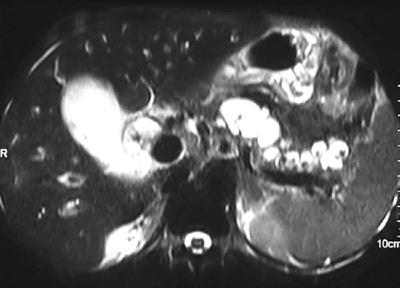

9) Cluster sign
10) Colon cut off

11) Comet-tail artifact
12) Cottage loaf sign

14) Crescent sign

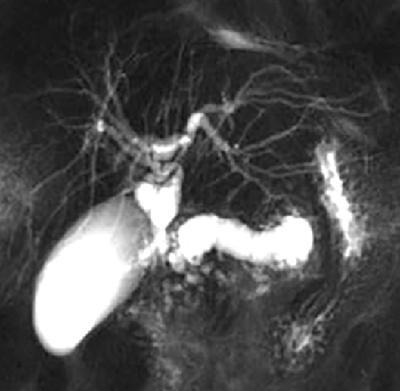
15) The double duct sign
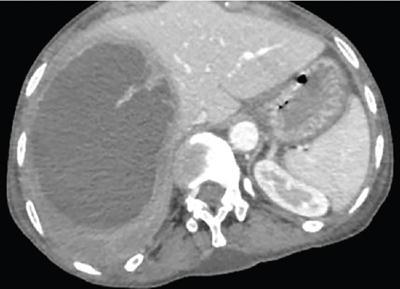
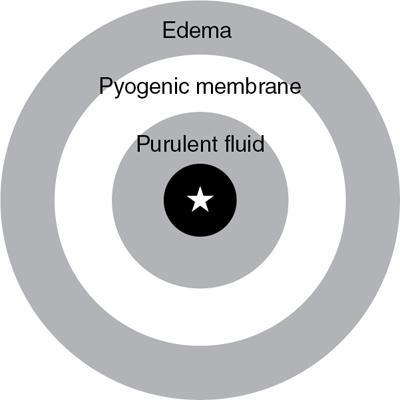
16) The double target sign
17) Duct penetrating sign
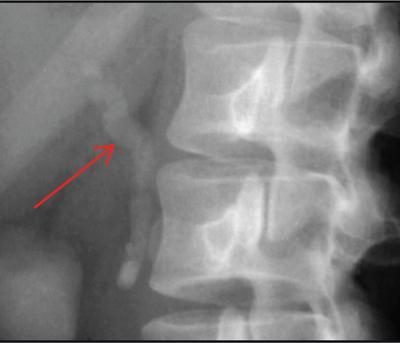
18) Exclamation mark sign

19) Enucleation sign
20) Expanded gallbladder fossa sign

21) Focal hepatic hot spot sign
22) Gallbladder ghost triad
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access






