Chapter 7 Recognizing Pneumonia
General Considerations
 Pneumonia can be defined as consolidation of lung produced by inflammatory exudate, usually as a result of an infectious agent.
Pneumonia can be defined as consolidation of lung produced by inflammatory exudate, usually as a result of an infectious agent.



 Because many different microorganisms can produce similar imaging findings in the lungs, it is difficult to identify with certainty the causative organism from the radiographic presentation alone.
Because many different microorganisms can produce similar imaging findings in the lungs, it is difficult to identify with certainty the causative organism from the radiographic presentation alone.• However, certain patterns of disease are very suggestive of a particular causative organism (Table 7-1).
TABLE 7-1 PATTERNS THAT MIGHT SUGGEST A CAUSATIVE ORGANISM
| Pattern of Disease | Likely Causative Organism |
|---|---|
| Upper lobe cavitary pneumonia with spread to the opposite lower lobe | Mycobacterium tuberculosis (TB) |
| Upper lobe lobar pneumonia with bulging interlobar fissure | Klebsiella pneumoniae |
| Lower lobe cavitary pneumonia | Pseudomonas aeruginosa or anaerobic organisms (Bacteroides) |
| Perihilar interstitial disease or perihilar airspace disease | Pneumocystis carinii (jiroveci) |
| Thin-walled upper lobe cavity | Coccidioides (Coccidiomycosis), TB |
| Airspace disease with effusion | Streptococci, staphylococci, TB |
| Diffuse nodules | Histoplasma, Coccidioides, Mycobacterium tuberculosis (histoplasmosis, coccidiomycosis, TB) |
| Soft-tissue, fingerlike shadows in upper lobes | Aspergillus (allergic bronchopulmonary aspergillosis) |
| Solitary pulmonary nodule | Cryptococcus (cryptococcosis) |
| Spherical soft-tissue mass in a thin-walled upper lobe cavity | Aspergillus (aspergilloma) |
General Characteristics of Pneumonia
• Because pneumonia fills the involved airspaces or interstitial tissues with some form of fluid or inflammatory exudate, pneumonias appear denser (whiter) than the surrounding, normally aerated lung.
• Pneumonia may contain air bronchograms if the bronchi themselves are not filled with inflammatory exudate or fluid (see Fig. 3-3).
• Air bronchograms are much more likely to be visible when the pneumonia involves the central portion of the lung near the hilum. Near the periphery of the lung, the bronchi are usually too small to be visible (Fig. 7-1).


 Except for the presence of air bronchograms, airspace pneumonia is usually homogeneous in density (Fig. 7-2).
Except for the presence of air bronchograms, airspace pneumonia is usually homogeneous in density (Fig. 7-2).

Box 7-1 Recognizing a Pneumonia—Key Signs
In airspace disease, the margins may be fluffy and indistinct except where they abut a pleural surface like the interlobar fissures where the margin will be sharp.
Interstitial pneumonias will cause a prominence of the interstitial tissues of the lung in the affected area; in some cases, the disease can spread to the alveoli and resemble airspace disease.
Patterns of Pneumonia
 Pneumonias may be distributed in the lung in several patterns described as lobar, segmental, interstitial, round, and cavitary (Table 7-2).
Pneumonias may be distributed in the lung in several patterns described as lobar, segmental, interstitial, round, and cavitary (Table 7-2).
TABLE 7-2 PATTERNS OF APPEARANCE OF PNEUMONIAS
| Pattern | Characteristics |
|---|---|
| Lobar | Homogeneous consolidation of affected lobe with air bronchogram |
| Segmental (bronchopneumonia) | Patchy airspace disease frequently involving several segments simultaneously; no air bronchogram; atelectasis may be associated |
| Interstitial | Reticular interstitial disease usually diffusely spread throughout the lungs early in the disease process; frequently progresses to airspace disease |
| Round | Spherically shaped pneumonia usually seen in the lower lobes of children that may resemble a mass |
| Cavitary | Produced by numerous microorganisms, chief among them being Mycobacterium tuberculosis |
Lobar Pneumonia
 The prototypical lobar pneumonia is pneumococcal pneumonia caused by Streptococcus pneumoniae (Fig. 7-3).
The prototypical lobar pneumonia is pneumococcal pneumonia caused by Streptococcus pneumoniae (Fig. 7-3).




Segmental Pneumonia (Bronchopneumonia)
 The prototypical bronchopneumonia is caused by Staphylococcus aureus. Many gram-negative bacteria, such as Pseudomonas aeruginosa, can produce the same picture.
The prototypical bronchopneumonia is caused by Staphylococcus aureus. Many gram-negative bacteria, such as Pseudomonas aeruginosa, can produce the same picture.
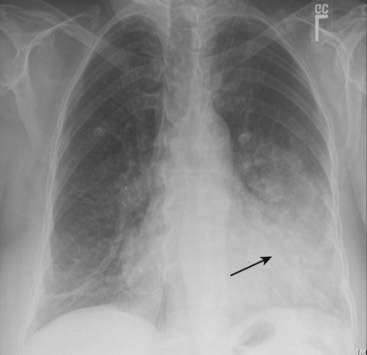
 Because lung segments are not bound by fissures, all of the margins of segmental pneumonias tend to be fluffy and indistinct (Fig. 7-4).
Because lung segments are not bound by fissures, all of the margins of segmental pneumonias tend to be fluffy and indistinct (Fig. 7-4).



