Chapter 8 Recognizing Pneumothorax, Pneumomediastinum, Pneumopericardium, and Subcutaneous Emphysema
Recognizing A Pneumothorax
 A pneumothorax occurs when air enters the pleural space.
A pneumothorax occurs when air enters the pleural space.• When this occurs, the negative pressure normally present in the pleural space rises higher than the intralveolar pressure and the lung collapses.
• The parietal pleura remains in contact with the inner surface of the chest wall, but the visceral pleura retracts toward the hilum with the collapsing lung.
• The visceral pleura becomes visible as a thin, white line outlined by air on both sides, marking the outer border of the lung and indicating the presence of the pneumothorax. The visible visceral pleura is called the visceral pleural white line or simply the visceral pleural line.
 You must be able to identify the visceral pleural line (Fig. 8-1) to make the definitive diagnosis of a pneumothorax!
You must be able to identify the visceral pleural line (Fig. 8-1) to make the definitive diagnosis of a pneumothorax!
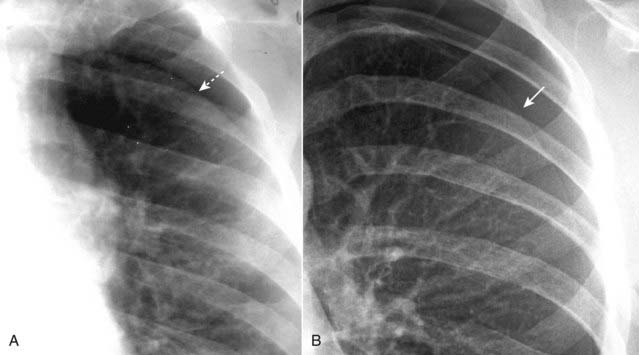
 Even as the lung collapses, it tends to maintain its usual lunglike shape so that the curvature of the visceral pleural line parallels the curvature of the chest wall; that is, the visceral pleural line is convex outward toward the chest wall (Fig. 8-2).
Even as the lung collapses, it tends to maintain its usual lunglike shape so that the curvature of the visceral pleural line parallels the curvature of the chest wall; that is, the visceral pleural line is convex outward toward the chest wall (Fig. 8-2). There is usually, but not always, an absence of lung markings peripheral to the visceral pleural line.
There is usually, but not always, an absence of lung markings peripheral to the visceral pleural line.

 Pitfall: Pleural adhesions may keep part, but not all, of the visceral pleura adherent to the parietal pleura, even in the presence of a pneumothorax (Fig. 8-3).
Pitfall: Pleural adhesions may keep part, but not all, of the visceral pleura adherent to the parietal pleura, even in the presence of a pneumothorax (Fig. 8-3).
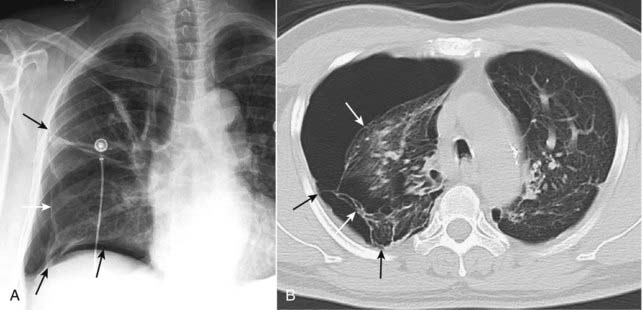
• On conventional radiographs, it may be possible to visualize lung markings in front or in back of the pneumothorax and to overlook the presence of a pneumothorax because lung markings appear to extend to the chest wall.
 The presence of an air-fluid interface in the pleural space is, by definition, an indication that a pneumothorax is present (see Fig. 6-14).
The presence of an air-fluid interface in the pleural space is, by definition, an indication that a pneumothorax is present (see Fig. 6-14).

Recognizing the Pitfalls in Overdiagnosing A Pneumothorax
 Several pitfalls can lead to the mistaken diagnosis of a pneumothorax.
Several pitfalls can lead to the mistaken diagnosis of a pneumothorax. Pitfall 1: Absence of lung markings mistaken for a pneumothorax.
Pitfall 1: Absence of lung markings mistaken for a pneumothorax.
• The simple absence of lung markings is not sufficient to warrant the diagnosis of a pneumothorax as other diseases produce such a finding.
• In none of these diseases would the treatment ordinarily include the insertion of a chest tube. In fact, insertion of a chest tube into a bulla might actually produce an intractable pneumothorax.
• Solution: Look at the contour of the structure you believe is the visceral pleural line. Unlike the margin of a bulla, the visceral pleural line will be convex outward toward the chest wall and will parallel the curve of the chest wall (Fig. 8-6).


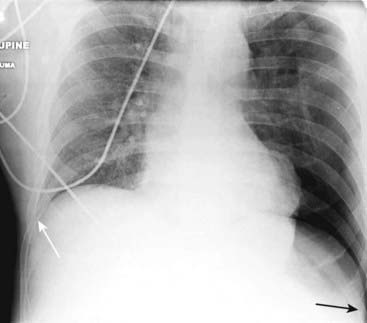
 Pitfall 2: Mistaking a skin fold for a pneumothorax.
Pitfall 2: Mistaking a skin fold for a pneumothorax.• When the patient lies directly on the radiographic cassette (as for a portable supine radiograph), a fold of the patient’s skin may become trapped between the patient’s back and the surface of the cassette.
• This can produce an edge in the expected position of the visceral pleural line which may, in fact, parallel the chest wall just as you would expect the visceral pleural line in a pneumothorax (Fig. 8-7).