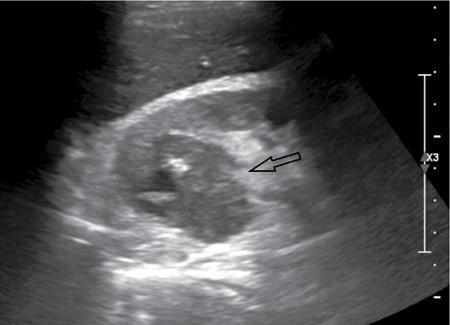
Renal abscess, like any other abscess in the body, is a localized collection of infective fluid in the kidney. It is usually a sequela of acute pyelonephritis, and a renal abscess should be suspected when appropriate antibiotic therapy does not lead to clinical response. It can affect all ages and has no recognized gender predilection. Abscess cavities may be either intra- or extraparenchymal. The most common clinical signs or symptoms encountered in renal and perinephric abscesses include fever with or without chills, flank/abdominal pain and dysuria. Renal abscess may be caused by either an ascending infection of the urinary tract or the haematogenous spread of a bacterial pathogen. Severe vasospasm and inflammation in the setting of advanced or inadequately treated cases of acute pyelonephritis may occasionally result in liquefactive necrosis and coalescence of multiple microabcesses to form renal abscess. A perinephric abscess may result from rupture of renal abscess into the perirenal space or direct involvement of perinephric space from inflammatory diseases of pancreas, colon and retroperitoneum. Diabetic patients are predisposed to abscess formation, with 75% of all renal abscesses occurring in this patient population. In addition, these patients can have an insidious presentation because of lack of flank pain related to diabetic neuropathy. Up to 15%–20% of patients with a renal abscess have negative urine cultures reflecting the fact that the infection has been relatively contained within a focal process. Fig. 10.12.2.4.1 summarizes the aetiology and predisposing factors of renal abscesses. In a case of renal and perirenal abscess, plain X-ray abdomen may show renal enlargement, rotation of renal axis, renal displacement, presence of mottled gas in renal areas and loss of psoas outline. The role of IVU in complicated pyelonephritis and renal abscess is rapidly diminished with the advent of superior imaging modalities such as ultrasound and CT scan. IVU generally shows poorly or nonfunctioning kidney with calyceal attenuation and compression due to mass effect. Typically shows a hypoechoic, walled-off collection with internal debris, increased through transmission of sound and no internal colour Doppler signals. Air within is visualized as nondependent echoes with dirty shadowing. However, diagnosis of abscess on sonography is not always straight forward as it can present as echogenic masses. Thus, a contrast-enhanced CT scan becomes essential for diagnosis. Moreover, CT is more sensitive than sonography for assessing spread to the perirenal space. CT is currently the most accurate modality for detection and follow-up of renal abscesses. Two imaging patterns are seen:
4. Renal and perinephric abscess
Introduction
Etiopathogenesis
Imaging findings
Plain radiograph
Intravenous urogram (IVU)
Ultrasound (Fig. 10.12.2.4.2)
CT
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


